You are called to see a 7-year-old with acute abdominal pain
Patient
Gender: male
Age: 7 years
Weight: 60 lb/27.2 kg
Height: 49 in/124 cm
Vitals
Temperature: 98 F/36.7 C
Blood Pressure: 125/79
Heart Rate: 112
Respiratory Rate: 28
Pulse Oximetry: 96% RA
Signs and Symptoms
2d RLQ abdominal pain; 103 F fever; nausea/vomiting
Click here to work through this patient case simulation.
Patient will present as → a 14-year-old boy with nausea, vomiting, constipation, and periumbilical pain that has settled in the lower right quadrant. The patient’s mom gave him a piece of toast and some water about 5 hours ago but he vomited 30 minutes after eating. On physical exam, he has tenderness and guarding in the lower right quadrant, pain upon flexion and internal rotation of right lower extremity, RLQ pain with right hip extension, and RLQ pain with palpation of the LLQ. Blood tests reveal leukocytosis with a shift to the left.
The first symptom is crampy or "colicky" pain around the navel (periumbilical) → then pain over McBurney’s point (RLQ)
There is usually a marked reduction in or total absence of appetite, often associated with nausea, and, occasionally, vomiting and low-grade fever
Most common etiology ⇒ fecalith
As the inflammation increases, the abdominal pain tends to move downward - begins in epigastrium → umbilicus → RLQ
Right lower quadrant= "McBurney's point." This "rebound tenderness" suggests inflammation has spread to the peritoneum
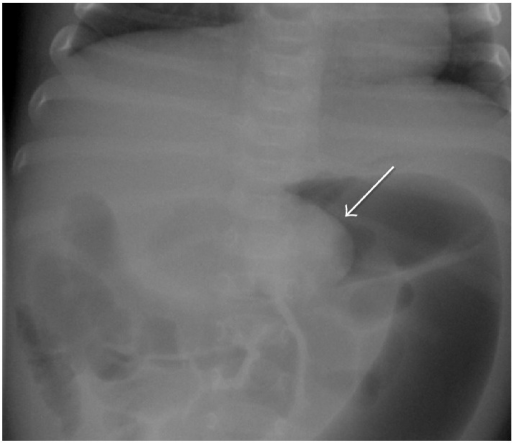
An abdominal x-ray will reveal a “Crescent sign” or a “Bull's eye/target sign/coiled spring lesion,” representing layers of the intestine within the abdomen
A barium enema is both diagnostic and therapeutic in children
Crescent sign of intussusception (image by Case Reports in Pediatrics CC BY 4.0)
An intraoperative ultrasound showing the classic target sign appearance of intussusception (image by open access)
You are called to see a 61 y/o with acute onset severe abdominal pain and vomiting
Patient
Gender: Female
Age: 61
Vitals
Temperature: 99.4ºF/37.4ºC
Heart Rate: 67
Respiratory Rate: 16
Pulse Oximetry: 99% on RA
Blood Pressure: 130/79
Signs and Symptoms
Acute onset severe abdominal pain and vomiting
Click here to work through this patient case simulation.
Patient with small bowel obstruction will present as → a 55-year-old male presents to the emergency department with a two-day history of severe abdominal pain, vomiting, and inability to pass stool or gas. He describes the pain as crampy and worsening, localized initially around the umbilicus but now diffused across the abdomen. His medical history is significant for an open appendectomy 20 years ago. On examination, his abdomen is distended and tender with high-pitched, tinkling bowel sounds. He is afebrile, but his heart rate is elevated. An abdominal X-ray reveals dilated loops of small bowel with air-fluid levels. You notevalvulae conniventes across the full width of the bowel suggestive of a small bowel obstruction. A CT scan of the abdomen confirms the diagnosis, showing a transition point with no evidence of strangulation. The patient is admitted for nasogastric decompression, intravenous fluids, and bowel rest. Surgery is consulted for potential operative intervention, given his history of previous abdominal surgery and the likelihood of adhesive disease. The patient is closely monitored for signs of bowel ischemia or perforation.
What are the 4 cardinal signs of strangulated bowel?
The 4 cardinal signs of strangulated bowel: fever, tachycardia, leukocytosis, and localized abdominal tenderness.
Small bowel obstruction
MCC: Postoperative adhesions (MC cause in adults) or hernias, cancer, IBD, volvulus, and intussusception(MC cause in children)
Obstruction is typically in the ileum or jejunum
History of prior abdominal surgery
Symptoms include colicky abdominal pain, nausea, biliousvomiting, abdominal distention, and diarrhea
DX: Obtain plain radiographs to quickly confirm a diagnosis of bowel obstruction, and, provided the films do not have findings that indicate the need for immediate intervention, then use computed tomography (CT) of the abdomen and pelvis to further characterize the nature, severity, and potential etiologies of the obstruction
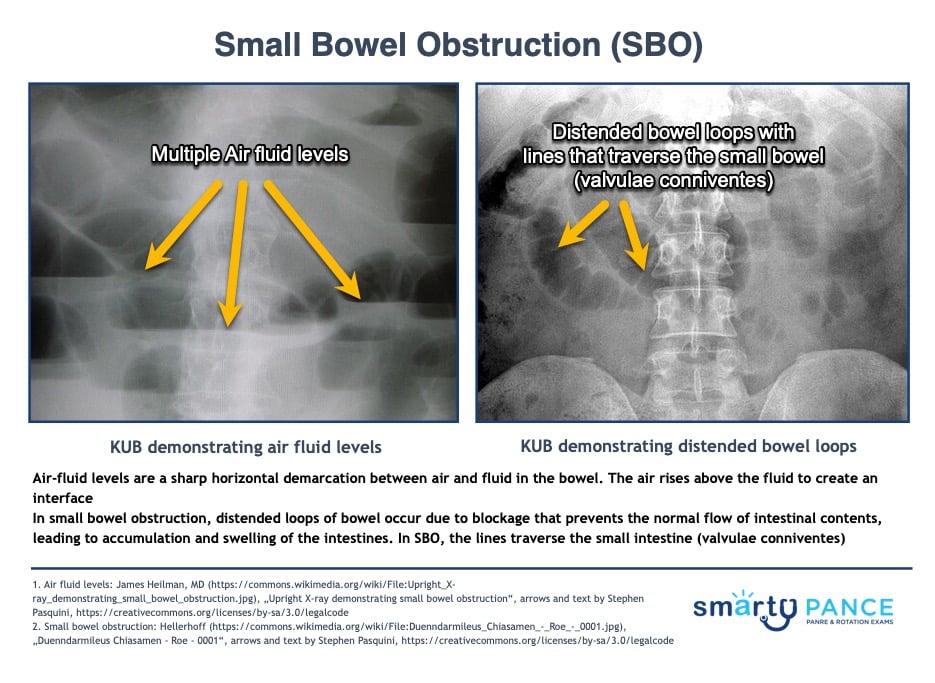
KUB shows dilated small bowel loops (< 3 cm), air-fluid levels in the small bowel with valvulae conniventes visible across the full width of the bowel, string of pearls (multiple air-fluid levels), and paucity of gas in the colon
TX: Treat with decompression with an NGT, bowel rest, surgery if a mechanical obstruction is suspected
Hyperactive bowel sounds, as heard in SBO
SBO vs. LBO
On the physical exam:
In small bowel obstruction, vomiting is more common, and the pain tends to be periumbilical, cramping, and intermittent – with bouts that last for a few minutes at a time
In large bowel obstruction, vomiting is less common, and the pain is lower in the abdomen and the bouts of pain are less frequent but last a bit longer
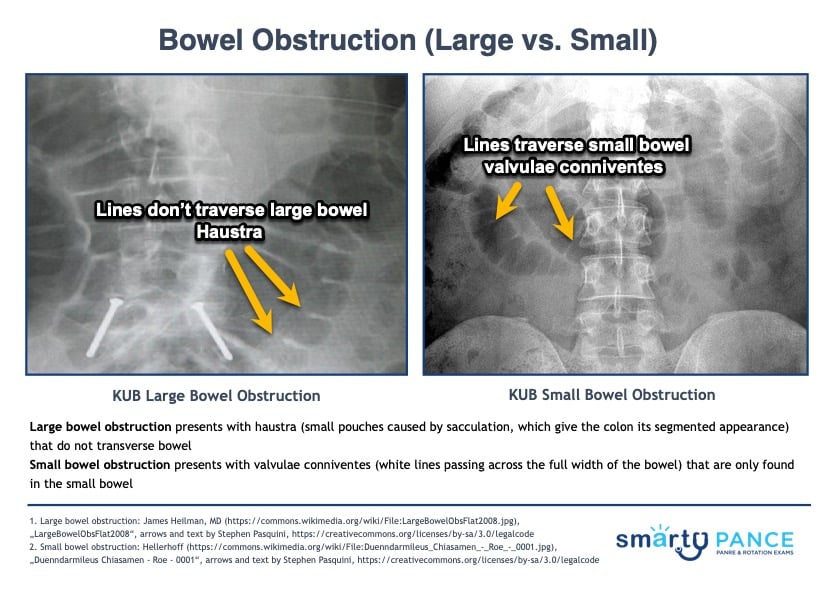
On the abdominal x-ray (KUB):
Large bowel obstruction presents with haustra (small pouches caused by sacculation, which give the colon its segmented appearance) that do not transverse bowel
Small bowel obstruction presents with valvulae conniventes (white lines passing across the full width of the bowel) that are only found in the small bowel
Patient will present as → a 45-year-old woman presents with intermittent, crampy abdominal pain and iron-deficiency anemia. She experiences occasional nausea but no vomiting, weight loss, or bowel habit changes. Her medical history and physical examination, including a soft, non-distended abdomen, are unremarkable. Despite normal upper endoscopy and colonoscopy results, persistent symptoms and anemia lead to a capsule endoscopy, revealing a 2 cm jejunal polyp. A double-balloon enteroscopy confirms it as a benign hamartomatous polyp. She undergoes successful endoscopic polypectomy, resolving her symptoms and anemia, with planned follow-up for symptom monitoring.
Small bowel polyps are abnormal growths of tissue protruding from the lining of the small intestine
Small bowel polyps are relatively uncommon, accounting for only about 3% of gastrointestinal tumors
Most small bowel polyps do not cause any symptoms. However, some people may experience abdominal pain, bloating, diarrhea, or bleeding (anemia)
DX: Small bowel polyps are often found incidentally during endoscopy, surgery, or imaging for other indications
Capsule endoscopy and device-assisted enteroscopy (double balloon or spiral) allow direct visualization of the small bowel
CT and MRI enterography
Biopsy during endoscopy provides definitive diagnosis based on histopathology
TX: Most small hyperplastic polyps can just be followed without intervention
Pedunculated or large adenomas should be removed via polypectomy during enteroscopy
For multiple polyps, consider surgical resection if accessible
Surveillance endoscopy is recommended after polypectomy due to risk of metachronous polyps
Malignant polyps require oncologic resection with lymph node dissection and possible chemotherapy




{kind=link}
{kind=link}