Patient will present as → a 26-year-old with a lesion on her tongue. For the last 4 months, she observed an alteration on the right side of the tongue, displaying alarming growth over a three-week period. The lesion is painful when the patient moves her tongue or while eating. She further mentions a recurrent, poorly healing aphthae on the right side of the tongue for a period of months before the current symptoms presented. On examination, the patient shows a symmetric face and normal skin color. Motor and sensory cranial nerve functions are within the normal range. No lymph nodes are palpable in her neck on both sides. On intraoral examination, you note a 15 x 20m exophytic lesion with a central ulcer appearing to infiltrate the tongue musculature that appears to be relatively well-demarcated.
{kind=link}
- Thyroid neoplastic disease (blueprint endocrinology): Papillary is the most common type
- Oral Cancer: Most often squamous cell carcinoma (blueprint dermatology) - It has been estimated that the use of tobacco and alcohol account for up to 80 percent of cases of squamous cell carcinoma of the head and neck
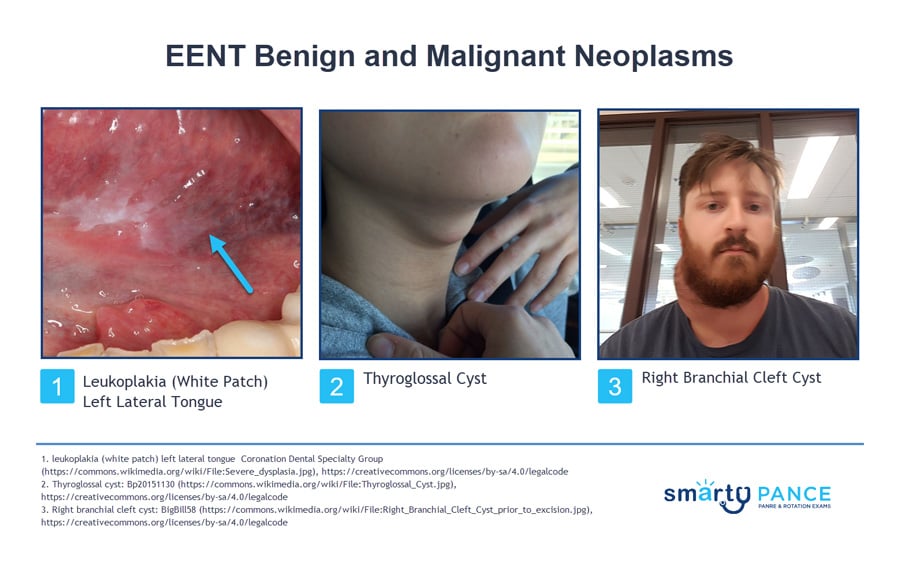
- Branchial Cleft Cyst: Cyst appearing after URI anterior to sternocleidomastoid, most common lateral neck mass
- Thyroglossal duct cyst: Hyoid or sub-hyoid soft mass that rises with tongue protrusion - most common midline neck mass
- Lymphadenopathy: Unilateral, painless, persistent, and cervical-think lymphoma (blueprint hematology)
- Leukoplakia: A white oral lesion that is painless and cannot be rubbed or scraped off. Lesions are often linked with tobacco, alcohol, or denture use. About 5% are dysplastic or squamous cell carcinomas. If there is an associated erythematous appearance (erythroplakia), there is a higher risk of dysplasia or cancer (90%)
{kind=link}
{kind=link}
Thyroid nodules: Lesions larger than 1 cm should be biopsied
Oral cancer: Persistent papules, plaques, erosions, or ulcers in the mouth should be biopsied to rule out squamous cell carcinoma, particularly in patients with appropriate risk factors.
Lymphoma: Other causes of lymphadenopathy should be excluded, such as syphilis, HIV, and mononucleosis. Persistent, unexplained, enlarged nodes should be biopsied. Reed–Sternberg cells confirm the diagnosis of Hodgkins Lymphoma
Leukoplakia: Leukoplakia itself is a benign reactive process. However, between 1 and 20 percent of lesions will progress to carcinoma within 10 years
Treatment is based on etiology. Refer to the following blueprint lessons:
Question 1 |
Sun exposure Hint: Sun exposure is a risk factor for cancer of the lip, but is not considered a major risk factor for oral cancer. | |
Alcohol abuse | |
Occupational exposure Hint: While occupational exposures and presence of premalignant lesions, such as leukoplakia, are risk factors for development of oral cancer, they are not considered major risk factors. | |
History of oral candidiasis Hint: History of oral candidiasis has no correlation to development of oral cancer. |
Question 2 |
optic nerve Hint: A lesion in the optic nerve would result in loss of vision in the affected eye only and include loss of central vision. | |
optic chiasm | |
temporal optic radiation Hint: A lesion in the temporal optic radiation would produce superior contralateral quadrantanopia. | |
optic tract |
Question 3 |
cranial nerve III Hint: Cranial nerve III is involved in extraocular movement and controls opening of the eyelids but has no control over closing the eyelids. | |
cranial nerve V Hint: Cranial nerve V controls the motor function of the temporal and masseter muscles and facial sensation. It has no control over eyelid closure. | |
cranial nerve VII | |
cranial nerve IX |
Question 4 |
Excessive conjunctival edema Hint: Excessive edema of the conjunctiva is a feature of chemosis. | |
Ptosis Hint: Ptosis is not indicative of an optic nerve lesion. | |
Inability to gaze laterally Hint: Inability to gaze laterally would be due to paralysis of the lateral rectus muscle controlled by cranial nerve VI. | |
Afferent pupillary defect |
Question 5 |
Painful creamy-white patches overlying erythema Hint: Oral candidiasis is characterized by painful creamy white patches overlying erythema. | |
Red smooth surface tongue Hint: Red smooth tongue is characteristic of glossitis which is most commonly associated with nutritional deficiencies. | |
Small vesicles on an erythematous base Hint: Small vesicles on erythematous bases are characteristic of herpetic stomatitis. | |
White lesion that cannot be removed by rubbing |
Question 6 |
Amaurosis fugax Hint: See B for explanation. | |
Bitemporal hemianopia | |
Unilateral blindness Hint: See B for explanation. | |
Homonymous hemianopia Hint: See B for explanation. |
|
List |
References: Merck Manual · UpToDate