Benign prostatic hyperplasia: The Daily PANCE Blueprint
A 68-year-old male comes to the clinic because of urinary issues. He reports that he is scared to continue his twice-weekly trips to see his grandchildren who live about an hour away because he has had two accidents in the car over the last few months when he has wet himself. He reports sudden urinary urgency and an inability to hold on until he finds a toilet. He also reports getting up to urinate two or three times during the night. He has had no pain with urination and otherwise feels well. Dipstick urinalysis is normal. Which of the following is the best treatment for short- and long-term symptom relief?
A. 5-alpha reductase inhibitor
B. Phosphodiesterase-5 inhibitor
C. Combination alpha-1 adrenergic blocker and phosphodiesterase-5 inhibitor
D. Alpha-1-adrenergic receptor blocker
E. Combination alpha-1 adrenergic blocker and 5-alpha reductase inhibitor
Answer and topic summary
The answer is E, Combination alpha-1 adrenergic blocker and 5-alpha reductase inhibitor
- Moderate to severe benign prostatic hyperplasia is best treated with dual therapy: a 5-alpha reductase inhibitor and an alpha-1 adrenergic receptor blocker.
View blueprint lesson
Pearls
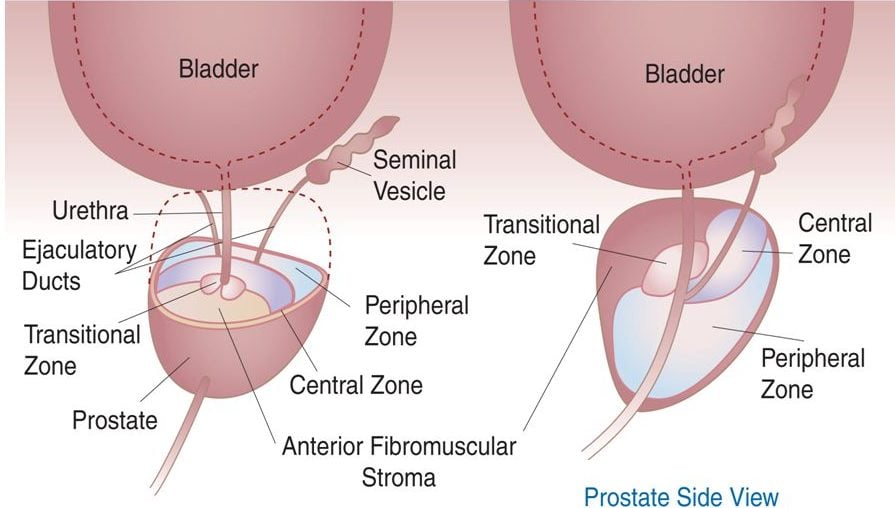
A disease of elderly men (average age is 60 to 65 years caused by hyperplasia of prostatic epithelial, stromal cells → formation of nodules in periurethral (transition) zone → narrowing of urethral canal → urethral compression → obstruction of the urinary outlet
- 50% of men develop BPH by 60 and > 90% by age 85
- Features: Decreased force of urinary stream, hesitancy (stop and start) and straining, postvoid dribbling, incomplete emptying, frequency, nocturia, urgency, recurrent UTIs
- In men with BPH avoid the use of anticholinergic and antihistamines
- This type of prostate enlargement isn’t thought to be a precursor to prostate cancer
Diagnosis
Accurately diagnosing BPH is extremely important as more serious conditions, such as prostate cancer must be ruled out
- DRE ⇒ enlarged rubbery prostate
- Urinalysis/Culture → Microscopic hematuria may be present → Pyuria, bacteriuria in case of concomitant UTI
- Blood tests → Often PSA often elevated > 4 → Electrolytes, blood urea nitrogen (BUN), and creatinine to evaluate for renal impairment
- Ultrasound → Evaluate bladder size, prostate size, degree of hydronephrosis
- Cystoscopy → Reveal bladder diverticula/calculi before scheduled invasive treatment
Treatment
Treatment includes medications that relax the bladder or shrink the prostate, surgery, and minimally invasive surgery
- Conservative measures; e.g. decrease fluid intake before bedtime/going out; avoid caffeine, alcohol (mild diuretic effects)
- Alpha-adrenergic receptor blockers (terazosin, tamsulosin) → decrease prostate, bladder, urethral muscle tone
- 5-alpha reductase inhibitors (finasteride) → decrease DHT synthesis → reduce prostate gland size
- Phosphodiesterase-5 enzyme inhibitors (e.g., tadalafil) → induce smooth muscle relaxation
- TURP (transurethral resection of the prostate) if refractory to meds → removes excess prostate tissue to relieve obstruction – sexual dysfunction and urinary incontinence
Smarty PANCE Content Blueprint Review:
Covered under ⇒ PANCE Blueprint Genitourinary (5%) ⇒ ⇒
{kind=link}