

A 31-year-old with anxiety, tremors, and hematemesis
Patient will present as → a 69-year-old male with a history of chronic alcohol use presents to the emergency department with sudden onset of severe epigastric pain radiating to the back that began 6 hours ago. He reports nausea and multiple episodes of vomiting. Vital signs show: BP 142/88 mmHg, HR 110 bpm, RR 22/min, temp 100.8°F. Physical exam reveals an unkempt, diaphoretic male in moderate distress with marked epigastric tenderness and guarding. His last alcoholic drink was approximately 18 hours ago. Laboratory studies show: lipase 850 U/L (normal <60), amylase 420 U/L (normal <100), and AST:ALT ratio of 3:1. The patient is made NPO, an NG tube is placed, and aggressive IV fluid resuscitation is initiated. On hospital day 2 (approximately 48 hours after his last drink), the patient develops visual hallucinations, tremors, and confusion. Shortly after, he experiences a generalized tonic-clonic seizure.
Key Points:
- Alcohol use disorder is divided into two:
- At-risk drinking: continuous use of alcohol (4 drinks/day or 14 drinks/week for men or 3 drinks/day or 7 drinks/week for women) to ameliorate symptoms of anxiety and emotional problems. According to CDC, a drink is defined as 12 oz of beer, 8 oz of malt liquor, 1.3 oz of hard liquor (spirits), or 5 Oz of wine.
- Moderate-severe drinking: recurrent use of alcohol despite personal, interpersonal and legal problems or risks.
DSM-5 Diagnostic Criteria
Alcohol Use Disorder DSM-5 Diagnostic Criteria
A problematic pattern of alcohol use leading to clinically significant impairment or distress, as manifested by at least two of the following, occurring within a 12-month period:
- Alcohol is often taken in larger amounts or over a longer period than was intended.
- There is a persistent desire or unsuccessful efforts to cut down or control alcohol use.
- A great deal of time is spent in activities necessary to obtain alcohol, use alcohol, or recover from its effects.
- Craving, or a strong desire or urge to use alcohol.
- Recurrent alcohol use resulting in a failure to fulfill major role obligations at work, school, or home.
- Continued alcohol use despite having persistent or recurrent social or interpersonal problems caused or exacerbated by the effects of alcohol.
- Important social, occupational, or recreational activities are given up or reduced because of alcohol use.
- Recurrent alcohol use in situations in which it is physically hazardous.
- Alcohol use is continued despite knowledge of having a persistent or recurrent physical or psychological problem that is likely to have been caused or exacerbated by alcohol.
- Tolerance, as defined by either of the following:
- A need for markedly increased amounts of alcohol to achieve intoxication or desired effect.
- A markedly diminished effect with continued use of the same amount of alcohol.
- Withdrawal, as manifested by either of the following:
- The characteristic withdrawal syndrome for alcohol
- Alcohol (or a closely related substance, such as a benzodiazepine) is taken to relieve or avoid withdrawal symptoms.
Alcohol Intoxication DSM-5 Diagnostic Criteria
- Recent ingestion of alcohol.
- Clinically significant problematic behavioral or psychological changes (e.g., inappropriate sexual or aggressive behavior, mood lability, impaired judgment) that developed during, or shortly after, alcohol ingestion.
- One (or more) of the following signs or symptoms developing during, or shortly after, alcohol use:
- Slurred speech.
- Incoordination.
- Unsteady gait.
- Nystagmus.
- Impairment in attention or memory.
- Stupor or coma.
- The signs or symptoms are not attributable to another medical condition and are not better explained by another mental disorder, including intoxication with another substance.
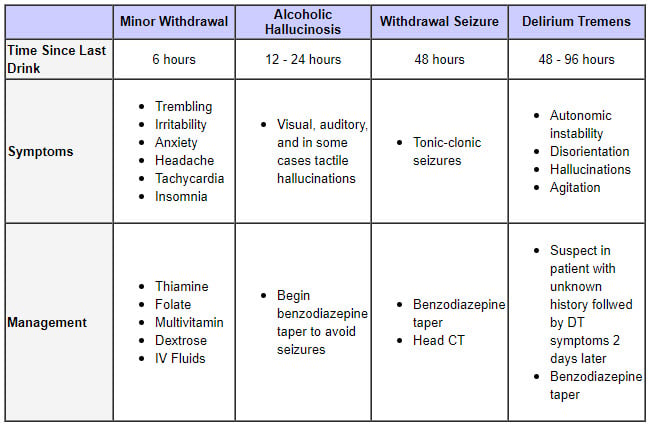
Alcohol Withdrawal DSM-5 Diagnostic Criteria
- Cessation of (or reduction in) alcohol use that has been heavy and prolonged.
- Two (or more) of the following, developing within several hours to a few days after the cessation of (or reduction in) alcohol use:
- Autonomic hyperactivity (e.g., sweating or pulse rate greater than 100 bpm).
- Increased hand tremor.
- Insomnia.
- Nausea or vomiting.
- Transient visual, tactile, or auditory hallucinations or illusions.
- Psychomotor agitation.
- Anxiety.
- Generalized tonic-clonic seizures.
- The signs or symptoms of withdrawal cause clinically significant distress or impairment in social, occupational, or other important areas of functioning.
- The signs or symptoms are not attributable to another medical condition and are not better explained by another mental disorder, including intoxication or withdrawal from another substance.
Treatment of at-risk drinking is multifactorial
- Psychological: motivational interviewing
- Social: social support from peers, family and organizations like Alcoholics Anonymous go a long way.
Addiction medications
- Disulfiram (Antabuse) - inhibits acetaldehyde dehydrogenase, aversive conditioning
- 500 mg once daily for 1-2 weeks then decrease to the maintenance dose (range 125-500 mg once daily)
- Nor for use in persons actively drinking alcohol; avoid alcohol in other products
- Oral Naltrexone - decreases desire
- 50 mg once daily
- Cannot be given to patients taking opioids
- Extended-Release Naltrexone - decreases desire
- 380 mg IM every 4 weeks; administer in the gluteal area with 1.5 inch 20-gauge needle
- Cannot be given to patients taking opioids
- Acamprosate - changes brain chemistry in a way that reduces anxiety, irritability, and restlessness associated with early sobriety
- 666 mg three times daily
- Dose reduction required with renal impairment
- Topiramate - reduces drinking at least as well as naltrexone and acamprosate
- Begin at 25 mg daily and increase up to 150 mg BID
- Gabapentin - decreases desire
- Begin at 300 mg once daily and increase up to 600 mg TID
Treatment of alcoholic hallucinosis involves the use of antipsychotics such as Haldol (5mg) with an appropriate taper.
Treatment of alcoholic withdrawal involves the use of benzodiazepines (long-acting such as diazepam) to depress the CNS excitation caused by the abrupt cessation of alcohol use. Fluid resuscitation, vitamins, thiamine, and electrolytes need to be replaced as well. NB: replace thiamine before giving any glucose-containing IV solutions in order to prevent Wernicke encephalopathy and Korsakoff psychosis.
Assessment of a client misusing alcohol requires knowledge of several key features and concerns. It is important to note that alcohol intoxication depresses the central nervous system (CNS), resulting in alterations in mentation, muscle coordination, and respiratory and cardiac function. With severe alcohol use, CNS depression may result in coma or death. A patient experiencing alcohol withdrawal may experience Wernicke-Korsakoff syndrome, which is characterized by Wernicke’s encephalopathy and Korsakoff’s psychosis. Alcohol use disorder may promote numerous medical complications including gastrointestinal irritation or bleeding, cardiomyopathy, pancreatitis, cirrhosis, immunosuppression, and sexual dysfunction.
Play Video + QuizAlcohol use disorder (interventions)
Alcohol is a neurotoxin that affects the brain in a complex manner from prolonged exposure and repeated withdrawal. Therefore, interventions for alcohol use disorder, dependence, and withdrawal are aimed at calming the patient and preparing for serious and possibly life threatening side effects of withdrawal, such as seizures, delirium tremens, hallucinations and even death. It also involves assessment to determine further risk factors for the patient, such as suicide. Medications, proper support systems, and group therapy are also important in the removal of dependence from alcohol.
Question 1 |
benzodiazepine | |
clonidine | |
barbiturates | |
anticonvulsants | |
all of the above
|
Question 2 |
a state in which a syndrome of drug-specific withdrawal signs and symptoms follows the reduction or cessation of drug use | |
a state in which the physiologic or behavioral effects of a constant dose of a psychoactive substance decrease over time
| |
a pathologic state that follows cessation or reduction in the amount of drug used
| |
a and b
| |
all of the above
|
|
List |