


5 y/o with new, pruritic, painful, vesicular rash
Patient with varicella (chickenpox) will present as → a 3-year-old with fatigue, irritability, and a low-grade fever that he has had for 3 days. According to the patient's mom, the child attends a daycare where a virus is “going around.” On physical examination, the child does not look ill. His temperature is 98.6 F (38 C). His skin examination shows scattered, small vesicles on an erythematous base. The rash was seen first on the face and seems to be spreading to the trunk.
{kind=link}

5 y/o with leg pain and rash
Patient with herpes zoster (shingles) will present as → a 67-year-old male who presents to your clinic with a two-day history of a painful rash on his left flank and radiating to his back. This was preceded by burning pain in the same region several days prior. The patient does not recall any history of childhood exanthems and is not up to date on his immunizations. Vital signs are stable. Physical exam reveals a maculopapular rash in a dermatomal distribution on the left flank and extending into the back.
{kind=link}
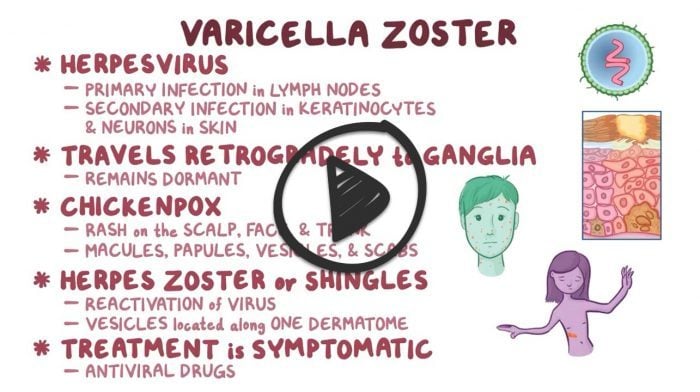
Varicella zoster virus (VZV) is one of the human herpes viruses (HHV3) that cause two diseases: 1. chickenpox (varicella) and 2. herpes zoster (shingles)
- Chickenpox follows initial exposure to the virus and is typically a relatively mild, self-limited childhood illness with a characteristic exanthem, but can become disseminated in immunocompromised children
- Reactivation of the dormant virus results in the characteristic painful dermatomal rash of herpes zoster, which is often followed by pain in the distribution of the rash (postherpetic neuralgia)
1. Varicella (Chicken Pox): primary infections - clusters of vesicles on an erythematous base - dew drops on a rose petal in different stages, starts on the face, and spreads down
- Varicella is transmitted by respiratory droplets and has a 10-20 day incubation period
- The vesicular rash of varicella, which is usually pruritic, appears in successive crops over several days. The lesions begin as macules that rapidly become papules followed by characteristic vesicles; these lesions can then develop a pustular component followed by the formation of crusted papules
- Typically has lesions in different stages of development on the face, trunk, and extremities
- New vesicle formation generally stops within four days, and most lesions have fully crusted by day six
- Crusts tend to fall off within about one to two weeks and leave a temporary area of hypopigmentation in the skin

A child presents with classic itchy red skin spots associated with the chickenpox virus.
2. Herpes Zoster (Shingles): varicella reactivation along one dermatome
- Pain, itching, or tingling in the area where the rash will develop
- A single stripe of vesicles around either left or right side of the body/one side of the face
- Four weeks for the rash to disappear ⇒ pain in affected dermatome > 90 days = postherpetic neuralgia
- Zoster ophthalmicus: shingles involving cranial nerve V (trigeminal nerve), dendritic lesions on slit lamp exam if keratoconjunctivitis is present
- Zoster Oticus (Ramsay-Hunt Syndrome): shingles involving facial nerve (CN VII) otalgia, lesions on the ear, auditory canal and TM, facial palsy auditory symptoms

A single stripe of vesicles around the right side of the body
Diagnosed clinically based on the way the skin lesions appear
- Herpes Zoster can be identified via tzanck smear with visualization of multinucleated giant cells
- Blood tests for varicella antibodies
- PCR to look for viral DNA (most sensitive and is more rapid (≤1 day) compared with conventional culture techniques)
- When PCR testing is not available, DFA testing is performed on scrapings from vesicular skin lesions that have not yet crusted and viral culture

Positive Tzanck test, showing three multinucleated giant cells in center.
.

"The Tzanck smear can detect multinucleated giant cells indicative of herpesvirus infections but lacks specificity for VZV and cannot distinguish between herpes simplex virus and VZV infections. When acute diagnostic confirmation is desired, modern tests, such as direct fluorescent antibody (DFA) testing or PCR (if available), are preferred to the Tzanck smear."
Varicella (chickenpox): symptomatic treatment (topical antipruritics and analgesics)
- Antivirals (acyclovir, famciclovir, valacyclovir) may be used in special populations.
- Aspirin should NOT be used ⇒ Reye syndrome
- Varicella-Zoster immune globulin (VZIG)
Varicella-zoster (shingles): acyclovir, famciclovir, valacyclovir given within 72 hours to prevent post-herpetic neuralgia
- Zoster ophthalmicus: oral antivirals, may add acyclovir ophthalmic
- Zoster oticus (Ramsay-Hunt Syndrome): oral acyclovir and corticosteroids
- Postherpetic neuralgia: Both gabapentinoids (ie, gabapentin and pregabalin) and tricyclic antidepressants (TCAs), topical lidocaine gel, capsaicin
Vaccination:
- Varicella Vaccine
- Children receive the first dose at age 12 through 15 months and the second dose at age 4 through 6 years
- People 13 years of age and older who have never had chickenpox or never received the chickenpox vaccine should get two doses, at least 28 days apart
- It is a live-attenuated vaccine:
- Pregnant women should not get chickenpox vaccine. They should wait to get the vaccine until after they have given birth
- Women should not get pregnant for 1 month after getting chickenpox vaccine.
- can be given to patients with HIV who have a CD4+ cell count greater than 200 cells/mm3
- Recombinant zoster vaccine (RZV, Shingrix) is recommended to prevent shingles in adults 50 years and older
- 2-dose series 2-6 months apart
- Should be given to patients who previously received Zostavax (ZVL) ⇒ administered at least two months after ZVL
 Osmosis Osmosis |
|
 |
Varicella-zoster virus (VZV) is third of the eight viruses in the herpesviridae family and is the cause of chicken-pox and shingles. This virus is an enveloped double-stranded linear DNA virus. Primary VZV infection results in chickenpox, which is a highly contagious illness that typically begins with a vesicular skin rash on the head and body. The rash is usually extremely itchy and can umbilicate and form scabs. Adults that get infected with primary infection commonly have more severe disease manifestations with more widespread rash and are more likely to experience complications such as pneumonia or encephalitis. Even when clinical symptoms resolve, the virus remains dormant in the trigeminal and dorsal root ganglia and can reactivate later in life to produce shingles, commonly called herpes zoster. Shingles is characterized by a painful blistering skin rash with a specific dermatome distribution on the body. Although the rash usually heals, some can suffer from residual nerve pain in a condition called postherpetic neuralgia. The organism can be identified via tzanck smear with visualization of multinucleated giant cells or the presence of cowdry A inclusions. Antiviral drugs like acyclovir can be used to reduce the severity and duration of VZV infection.
Play Video + QuizChickenpox

Chickenpox or varicella is a highly contagious communicable disease affecting children. It is communicable approximately 1 day before the eruption of the lesions to 6 days after the first crop of vesicles when crusts have formed. Typical incubation is 14-16 days. The disease is transmitted by direct contact [skin lesions, not the scabs], droplet (airborne) spread, and via contaminated objects.
Acyclovir (Zovirax)
Acyclovir (Zovirax) is an antiviral medication that inhibits viral replication in organisms of the herpes virus family. This medication is indicated for infections caused by herpes simplex virus and varicella zoster virus. This drug comes in several forms including topical, oral, and intravenous. Side effects of oral acyclovir include nausea, vomiting, diarrhea, and headache. Side effects of IV acyclovir include nephrotoxicity and neurotoxicity. Special considerations includes preventing recurring episodes of herpes simplex virus and administering IV acyclovir at a slow rate.
Play Video + QuizQuestion 1 |
Prednisolone Hint: There is no role for corticosteroids in the management of herpes zoster infection. | |
Valacyclovir | |
Laninamivir Hint: Laninamivir is a neuraminidase inhibitor which is being researched for the treatment and prophylaxis of Influenza virus A and Influenza virus B. It is currently in Phase III clinical trials | |
Lamivudine Hint: Is used to treat HIV and HBV infections |
Question 2 |
Gabapentin | |
Naproxen Hint: Is not recommended in the treatment of postherpetic neuralgia | |
Acetaminophen Hint: Is not recommended in the treatment of postherpetic neuralgia | |
Aspirin Hint: Is not recommended in the treatment of postherpetic neuralgia |
Question 3 |
Classic rash appearance is the “dew drop on a rose petal” Hint: The classic rash appearance is the “dew drop on a rose petal” | |
May be complicated by secondary bacterial skin superinfection Hint: Varicella may be complicated by a secondary bacterial skin infection | |
Incubation period is 5–7 days | |
Varicella-zoster vaccine is a live attenuated vaccine Hint: Varicella-zoster vaccine is a live attenuated vaccine. The varicella vaccine is given in two doses. A child should have the first shot at ages 12-18 months. The second shot should be given at ages 4-6 years. Older children and adults should have two shots, with four to eight weeks between the first and second shot. |
|
List |
References: Merck Manual · UpToDate