
Patient will present as → a 35-year-old G3P2 with cervical dilatation >3 cm, ruptured membranes, bleeding >7 days, and the presence of cramping (inevitable abortion)
Fetal death and early delivery are classified as follows:
- Abortion: Death of the fetus or passage of products of conception (fetus and placenta) before 20 weeks gestation
- Fetal demise (stillbirth): Fetal death after 20 weeks
- Preterm delivery: Birth of a live fetus between 20 weeks and 36 weeks + 6 days

"In modern clinical practice and patient-centered communication, the term miscarriage is preferred when referring to spontaneous (non-induced) pregnancy loss, as it is clearer and less stigmatizing for patients. The terms may be used interchangeably on exams depending on context. The terms may be used interchangeably on exams depending on context."
Classification of Abortion (Pregnancy Loss < 20 Weeks)
By Gestational Age
- Early: < 12 weeks
- Late: 12–20 weeks
By Etiology
- Spontaneous: Non-induced pregnancy loss
- Induced: Termination of pregnancy for medical or elective reasons
- Therapeutic: Termination due to maternal life/health risk or fetal anomalies incompatible with life
| Clinical Classification of Spontaneous Abortion (Miscarriage) | |
| Early | Abortion before 12 weeks gestation |
| Late | Abortion between 12 and 20 weeks gestation |
| Spontaneous | Noninduced abortion |
| Induced | Termination of pregnancy for medical or elective reasons |
| Therapeutic | Termination of pregnancy because the woman’s life or health is endangered or because the fetus is dead or has malformations incompatible with life |
| Threatened | Vaginal bleeding occurring before 20 weeks gestation without cervical dilation and indicating that spontaneous abortion may occur |
| Inevitable | Vaginal bleeding or rupture of the membranes accompanied by dilation of the cervix |
| Incomplete | Expulsion of some products of conception |
| Complete | Expulsion of all products of conception |
| Recurrent (habitual) | ≥ 2 to 3 consecutive spontaneous abortions |
| Missed | Undetected death of the fetus before 20 weeks of gestation, with products of conception remaining intrauterine |
| Septic | Serious infection of the uterine contents during or shortly before or after an abortion |
Recurrent Spontaneous Abortion (2-3 or more consecutive spontaneous abortions): Recommended Evaluation
- Genetic testing of parents
- Thyroid disorders (hypothyroidism or hyperthyroidism)
- Autoimmune conditions, including:
- Systemic lupus erythematosus (SLE)
- Antiphospholipid syndrome (anticardiolipin antibodies)
Spontaneous abortion:
- > 80% occur in the first trimester (< 12 weeks)
- ~60% are due to chromosomal abnormalities
- Remaining cases are often idiopathic
Increased Risk Factors
- Increasing parity
- Advanced maternal age (≥ 35) and paternal age (≥ 45)
- Conception within 3 months of a term delivery
- Cigarette smoking
- Substance use (alcohol, cocaine)
- Poorly controlled chronic maternal disease, including:
- Diabetes mellitus
- Hypertension
- Overt thyroid disorders
Diagnosed by ↓ βHG and classified based on ultrasound findings
- Transvaginal ultrasonography is the cornerstone of the evaluation of bleeding in early pregnancy
- The US demonstrates inappropriate development or interval growth, poorly formed/unformed fetal pole, and fetal demise
- The βHG should double every 48 hours in a viable intrauterine pregnancy
- Blood type and Rh status are necessary tests to preclude Rh sensitization in the mother
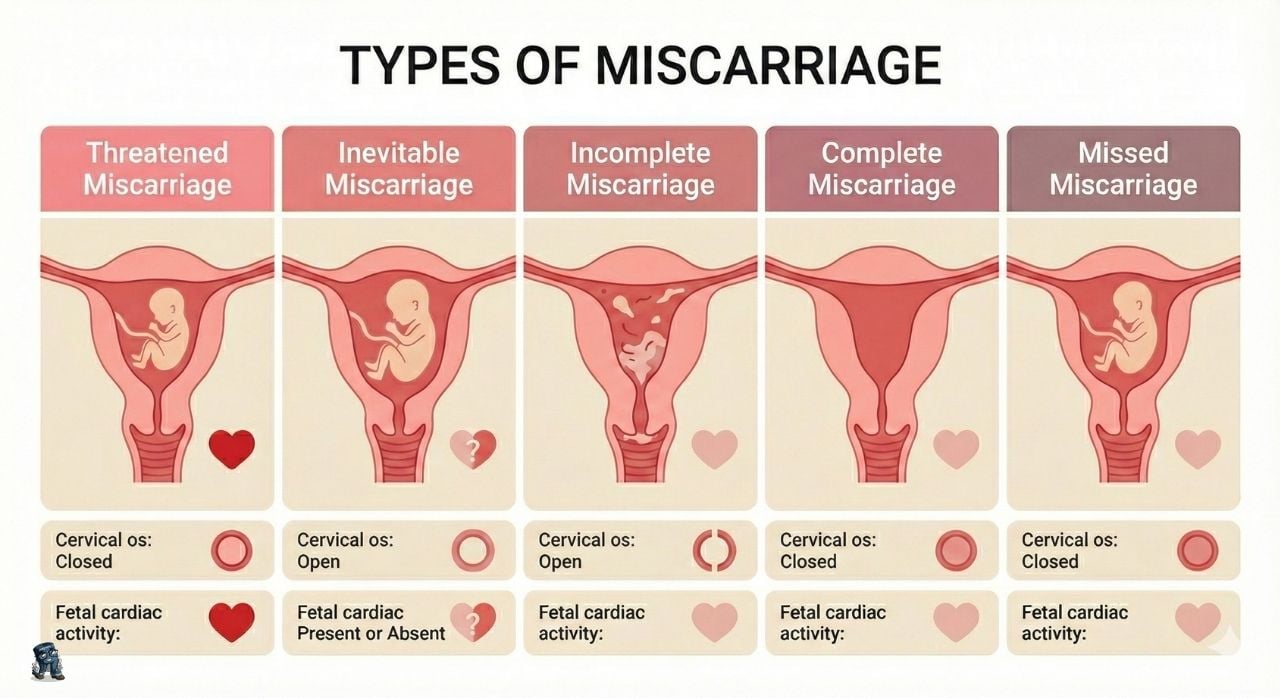
Miscarriage (Early Pregnancy Loss) Classifications
| Type | Bleeding | Cervical Os | Products of Conception | Key Clinical Feature |
|---|---|---|---|---|
| Threatened | Present | Closed | None passed | Viable intrauterine pregnancy |
| Inevitable | Present | Open | None passed | Miscarriage cannot be prevented |
| Incomplete | Present | Open | Some passed | Retained products remain |
| Complete | Resolved | Closed | All passed | Empty uterus on ultrasound |
| Missed | Minimal or none | Closed | None passed | Non-viable embryo or fetus |
Traditionally managed by D&C only, monitor progress with B-HCG levels or ultrasound examination
- Comprehensive management of early pregnancy loss includes addressing the emotions of women and their partners, inquiring about future plans for pregnancy, and offering contraceptive or preconception planning as appropriate
Elective abortion:
- Medical abortion: Mifepristone and Misoprostol up to first 7-9 weeks LMP
- Suction Curettage: safest and most effective for 12 weeks or less. Surgical procedure 3-12 weeks LMP. local anesthesia on the cervix
- Surgical Curettage (D&C) Aspiration: a surgical abortion up to 16 weeks LMP
- Dilation and Evacuation (D&E) up to 18 weeks outpatient
- Induction of labor with intraamniotic installation after 16 weeks
- Induction of labor with vaginal prostaglandins after 16 weeks
 Spontaneous abortion is defined as loss of pregnancy before 20 weeks gestation. Excessive bleeding before 20 weeks gestation in a pregnant women may indicate a nonviable fetus. Types of spontaneous abortion include threatened, inevitable, incomplete, complete, and missed. Identifying the type of spontaneous abortion is critical for determining subsequent treatment. Interventions include promoting bed rest and providing emotional support. Since fluid imbalance may occur in spontaneous abortion, monitoring for hemorrhage includes saving the patient’s pads and linens. The administration of RhoGAM may be necessary for Rh- women exposed to R+ blood of nonviable fetuses. Dilation & curettage and cerclage may be done to remove fetal tissue from inside the uterus.
Spontaneous abortion is defined as loss of pregnancy before 20 weeks gestation. Excessive bleeding before 20 weeks gestation in a pregnant women may indicate a nonviable fetus. Types of spontaneous abortion include threatened, inevitable, incomplete, complete, and missed. Identifying the type of spontaneous abortion is critical for determining subsequent treatment. Interventions include promoting bed rest and providing emotional support. Since fluid imbalance may occur in spontaneous abortion, monitoring for hemorrhage includes saving the patient’s pads and linens. The administration of RhoGAM may be necessary for Rh- women exposed to R+ blood of nonviable fetuses. Dilation & curettage and cerclage may be done to remove fetal tissue from inside the uterus.
| Spontaneous abortion types | Play Video + Quiz |
| Spontaneous abortion overview | Play Video + Quiz |
Question 1 |
uterine intramural myomata | |
progesterone deficiency elevated serum beta HCG | |
tobacco use | |
controlled diabetes |
Question 2 |
come to your office first thing in the morning for an evaluation | |
take some ibuprofen and see you at her next scheduled prenatal visit | |
rush to the emergency department because of suspected ectopic pregnancy | |
rush to the emergency department for an immediate dilation and curettage (D& C) | |
call an obstetrician-gynecologist to schedule an outpatient consultation |
Question 3 |
missed abortion | |
recurrent spontaneous abortion | |
complete abortion | |
incomplete abortion | |
inevitable abortion |
Question 4 |
expectant management | |
uterine aspiration | |
medical management with vaginal misoprostol | |
exploratory laparoscopy | |
serial β-human chorionic gonadotropin (β-hCG) measurements |
Question 5 |
Threatened abortion Hint: Threatened abortion is characterized by bleeding in the first trimester without loss of fluid or tissue. | |
Inevitable abortion | |
Incomplete abortion Hint: Complete abortion refers to a documented pregnancy that spontaneously passes all of the products of conception. | |
Incomplete abortion Hint: Incomplete abortion is when the cervical os is open and allows passage of blood. The products of conception may remain in utero or may partially extrude through the open os. |
|
List |
References: Merck Manual · UpToDate