 Lecture
LecturePatient with infectious mastitis presents as → a breastfeeding woman 3 weeks postpartum complaining of a painful area of the breast that is reddened and warm. The patient is very fatigued, with a fever of 101.5 °F and chills. She reports a burning pain present constantly or at times only while breastfeeding. On exam, the patient appears ill. Breast examination shows an erythematous right breast with a palpable mass, induration, erythema, and tenderness to palpation.
Patient with congestive mastitis presents as → a primigravida with bilateral, painful breast engorgement.

To watch this and all of Joe Gilboy PA-C's video lessons you must be a member. Members can log in here or join now.
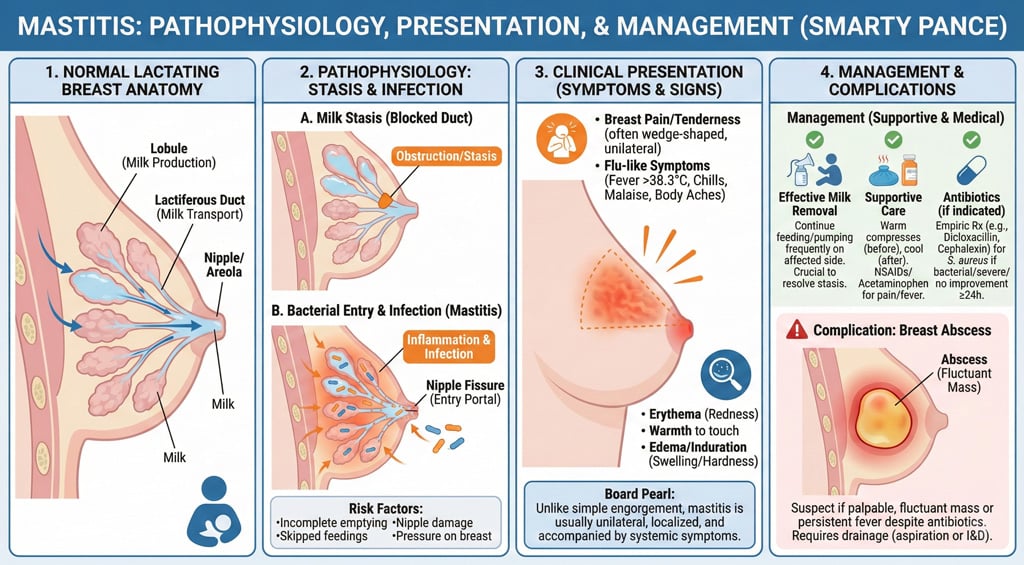 Mastitis is a condition in which bacteria enter the breast tissue through a milk duct or a fissure in the skin, caused by breastfeeding. Mastitis usually occurs within the first few weeks of breastfeeding, but may occur later
Mastitis is a condition in which bacteria enter the breast tissue through a milk duct or a fissure in the skin, caused by breastfeeding. Mastitis usually occurs within the first few weeks of breastfeeding, but may occur later
- Mastitis occurs mainly in breastfeeding women. Rarely, this condition occurs in women who are not breastfeeding
- Typically caused by Staphylococcus aureus, including MRSA in some cases
- Presents with localized breast pain, erythema, swelling, warmth, and tenderness; systemic symptoms like fever and malaise may also occur
- May progress to breast abscess—(palpable fluctuating mass)
- Infectious vs. congestive mastitis (unilateral vs. bilateral)
- Infectious (unilateral) - Unilateral, fever, chills, and color change
- Congestive (bilateral) - Bilateral breast engorgement that usually occurs in primigravidas. Diffuse breast tenderness, swelling, and firmness. No systemic symptoms (e.g., fever or chills)
***Inflammatory breast cancer presents with breast tenderness and color change, but fever and chills are not usually present
Diagnosis is clinical – if an abscess is suspected and ultrasound may be warranted
- Culture of the breast milk can be useful in guiding the selection of antibiotics
- Blood cultures are warranted in the setting of severe infection

Breast with mastitis
Treat with dicloxacillin 250 mg QID x 10 days for staphylococcus
- Patients should be encouraged to continue breastfeeding and apply warm/cold compresses to the infected area along with oral NSAIDs
Question 1 |
Cease breastfeeding and advise the mother to pump her breast milk until the infection resolves. Hint: Stopping breastfeeding is not necessary in cases of mastitis. Continuing to express milk helps with infection resolution and maintains milk supply. | |
Continue breastfeeding, and manage the mother's condition with warm compresses and antibiotics. | |
Maintain breast-feeding, administering antibiotics to both the mother and the infant. Hint: Treating both the mother and the infant with antibiotics is not typically required unless the infant shows signs of infection, which is rare. | |
Temporarily halt breastfeeding and start antibiotic therapy for the mother. Hint: Discontinuing breastfeeding is not recommended as the first line of action. Expressing milk from the affected breast is important to manage symptoms and clear the infection. | |
Stop all breastfeeding and proceed with incision and drainage of the affected area immediately. Hint: This procedure is reserved for abscess formation, which is a different condition and typically only considered if the infection does not respond to antibiotics and there is a collection of pus. |
Question 2 |
Evaluate the baby's latch-on technique and positioning during breastfeeding. Hint: Incorrectly assessing the baby's latch-on and the mother's positioning can lead to ineffective emptying of the breast, which is a common cause of mastitis. Proper technique is crucial for preventing milk stasis. | |
Suggest varying breastfeeding positions to ensure all milk ducts are being utilized. Hint: Using a variety of breastfeeding positions helps to ensure that all areas of the breast are being emptied, reducing the risk of milk stasis and subsequent infection. | |
Confirm the patient is well-rested, properly hydrated, and not delaying breastfeeding or pumping sessions excessively. Hint: Adequate rest and hydration are vital for maintaining a healthy milk supply, while regular feeding or pumping prevents the buildup of milk that can lead to infection. | |
Inspect the nipples for any signs of damage, such as cracks or fissures, and for evidence of a fungal infection. Hint: Nipple damage can serve as an entry point for bacteria, leading to mastitis. Identifying and treating any nipple issues promptly is essential for preventing recurrent infections. | |
All of the above |
|
List |
References: Merck Manual · UpToDate