Neoplasms of the Breast and Reproductive Tract
| Condition | Location & Features | Treatment |
| Benign | ||
| Fibroadenoma | Breast; mobile, firm, painless, well-circumscribed mass in young women | Observation or excision if symptomatic |
| Fibrocystic changes | Breast; cyclic breast pain, multiple cysts, often bilateral | Supportive care, NSAIDs, OCPs |
| Intraductal papilloma | Breast; bloody nipple discharge, no mass | Surgical excision |
| Breast abscess | Breast; painful, fluctuant mass with erythema, typically lactating women | I&D + antibiotics |
| Fibroid (leiomyoma) | Uterus; asymptomatic or menorrhagia, pelvic pressure | Observation, OCPs, myomectomy or hysterectomy |
| Endometrial hyperplasia (w/o atypia) | Uterus; postmenopausal bleeding, thickened endometrium | Progestin therapy, monitor with repeat biopsy |
| Ovarian cyst (functional) | Ovary; asymptomatic or pelvic pain, often resolves spontaneously | Observation or NSAIDs |
| Polycystic ovary syndrome (PCOS) | Ovary; multiple small cysts, irregular menses, hirsutism, insulin resistance | OCPs, metformin, weight loss |
| Hydatidiform mole (benign GTD) | Uterus; abnormal pregnancy with grape-like vesicles, ↑β-hCG | Suction D&C, monitor β-hCG |
| Malignant | ||
| Breast cancer (invasive ductal) | Most common (80%)
Breast; hard, immobile, irregular mass, nipple retraction, peau d’orange Spiculated mass or architectural distortion Often unifocal and unilateral |
Surgery, radiation, chemo, hormonal therapy |
| Breast cancer (invasive lobular) | Second most common (~10–15% of cases)
Breast; bilateral, multicentric, less likely to form a discrete mass Often diagnosed at later stage due to subtle findings |
Surgery + adjuvant therapy |
| Inflammatory breast cancer | Breast; rapid-onset breast erythema, edema (peau d’orange), no discrete mass, often tender and mistaken for mastitis; poor prognosis | Neoadjuvant chemotherapy, then mastectomy + radiation |
| Paget disease of the breast | Nipple/areola; eczematous lesion with underlying carcinoma | Mastectomy ± radiation |
| Endometrial carcinoma | Uterus; postmenopausal bleeding, abnormal ultrasound findings | Hysterectomy ± radiation or chemo |
| Ovarian cancer (epithelial) | Ovary; bloating, ascites, pelvic mass, often advanced at diagnosis | Surgery + chemo |
| Cervical intraepithelial neoplasia (CIN II/III) | Cervix; abnormal Pap smear, precancerous lesions | LEEP, ablation, or close monitoring |
| Cervical cancer (SCC) | Cervix; postcoital bleeding, friable lesion, HPV-related | Surgery, radiation, chemo |
| Choriocarcinoma | Uterus; malignant gestational trophoblastic disease (GTD), very high β-hCG, hemoptysis if metastases
Develops after a molar pregnancy, miscarriage, or abortion |
Chemotherapy (methotrexate or actinomycin D) |
| Vaginal carcinoma | Upper 1/3 posterior vaginal wall; painless vaginal bleeding, mass, or discharge; associated with HPV (16, 18) and often secondary to cervical or vulvar cancer | Radiation therapy ± surgical excision |
| Vulvar carcinoma | Vulva; pruritus, ulcerated or exophytic lesion, HPV or lichen sclerosus-related | Surgical excision ± radiation |
Malignant Reproductive Neoplasms
| Breast Cancer | Patient will present as → a 66-year-old female with concern over a mass she felt in her left breast on recent breast self-examination. She denies any nipple discharge and reports a negative family history of breast or other cancers. Physical examination confirms the presence of a painless, firm, irregular, and immobile lump in the superolateral quadrant of the left breast; there are no evident overlying skin changes, and there is no notable axillary lymphadenopathy on palpation. A mammogram is performed, with results seen here. Breast Cancer is the most common malignancy in women
Types:
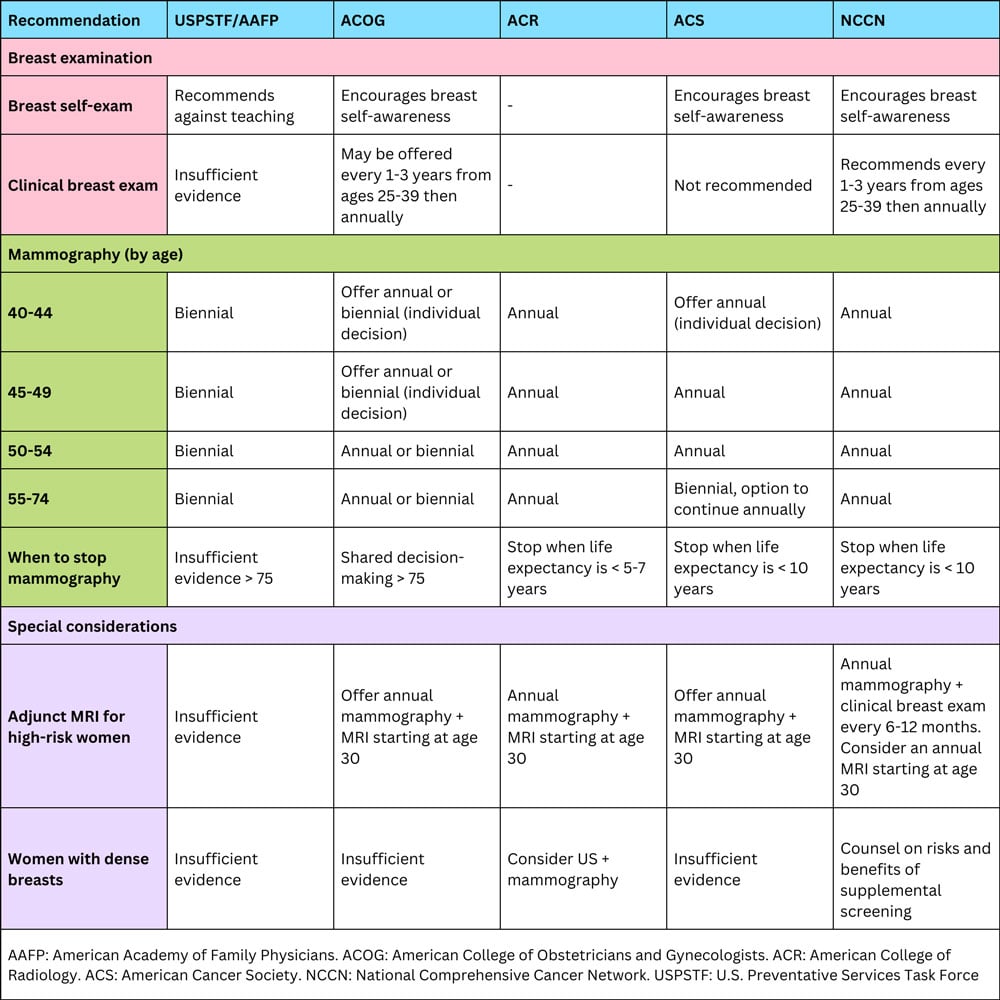
Tumors may be Estrogen receptor (ER) positive 75%, Progesterone receptor (PR) positive 65%, and HER2 positive 25% Mammography screening (USPSTF guidelines):
Average risk breast cancer screening guidelines:
Risk calculators for the average woman include: TX:
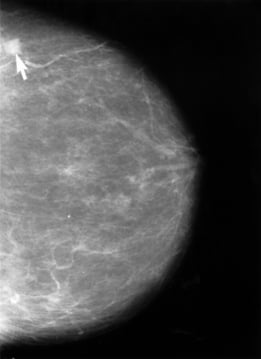 Mammogram demonstrating breast cancer. Image by NIH Senior Health via Wikimedia Commons, Public Domain. |
| Cervical cancer | Patient will present as → a 45-year-old female with post-coital bleeding and painful intercourse. On exam, you notice a friable, bleeding cervical lesion. The cytological evaluation shows a high-grade squamous intraepithelial lesion (HSIL/CIN2/3). She is referred for colposcopy and directed biopsies. Cervical cancer is the third most common type of cancer
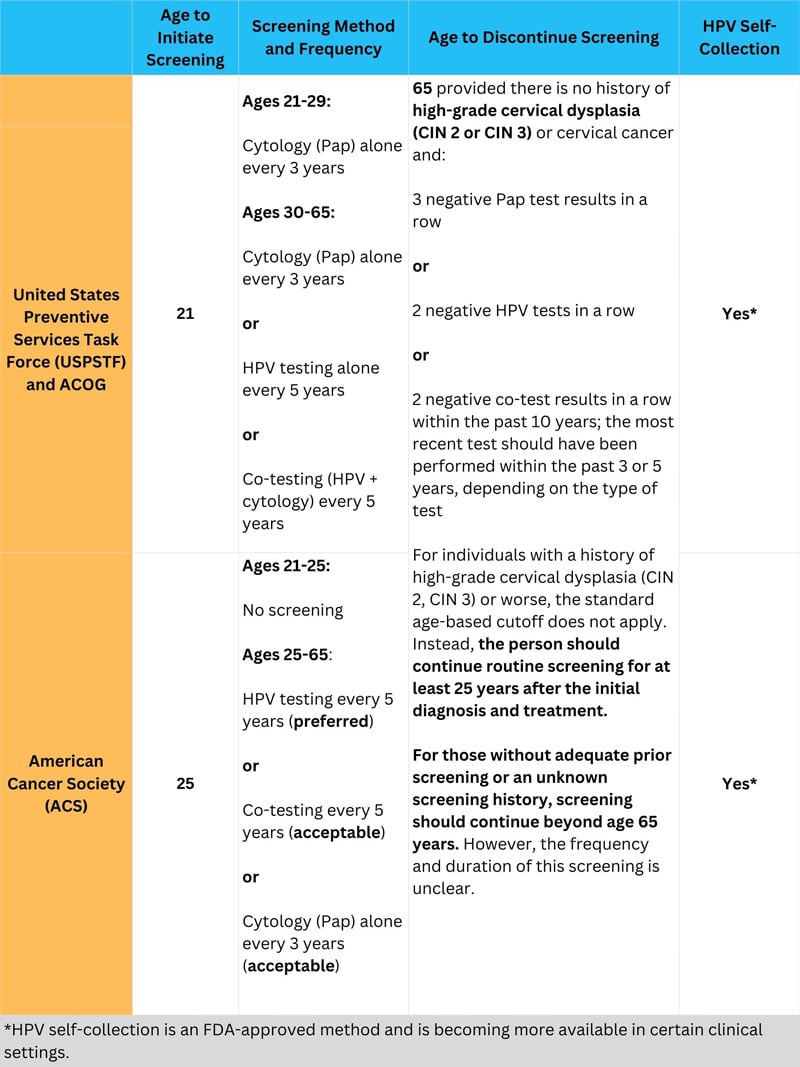
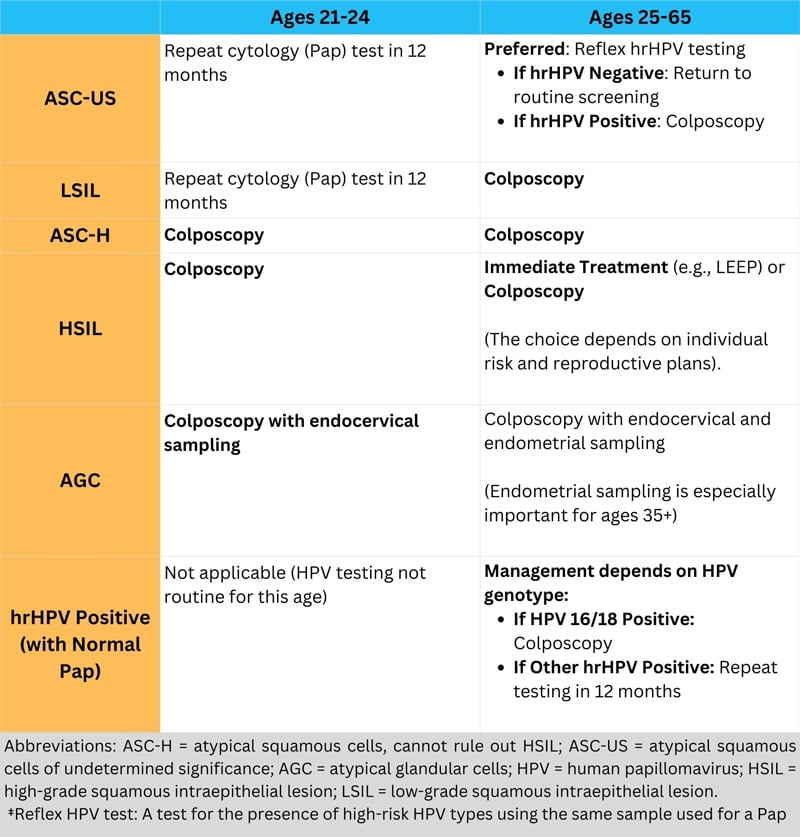
USPSTF guidelines for cervical cancer screening
DX: Friable, bleeding cervical lesion on exam
TX: Resect and/or chemotherapy and radiation
 DES-exposed cervix showing cervical structural changes. Image via Wikimedia Commons, public domain. |
| Ovarian Cancer | Patient will present as → a 66-year-old woman who complains of abdominal fullness, bloating, fatigue, and weight loss. She underwent menopause 17 years ago and has never had children. She had a pelvic mass, but her PAP smear is atrophic. CA-125 levels are elevated. A transvaginal ultrasound demonstrates an ovarian mass concerning for malignancy. Ovarian cancer is the second most common type of GYN cancer in women (the first is endometrial cancer)
DX: Diagnose with transvaginal ultrasound, then biopsy
TX: Stage 1A or 1B—Surgical excision alone (abdominal hysterectomy and bilateral salpingo-oophorectomy)
Preoperative transvaginal ultrasonography (a) detected an isoechoic solid mass in the right pelvic cavity (approximately 10 cm in size) with an ill-defined boundary between the lesion and the uterus, and T2-weighted magnetic resonance imaging of the ovarian tumor in (b) the horizontal and (c) the sagittal planes. The mass was later identified as a fibroma. Image by Diagnostic Pathology. License: CC BY 4.0 |
| Endometrial cancer | Patient will present as → a 53-year-old woman with no period for four years and is now having abnormal bleeding and bleeding after intercourse. She has lower abdominal pain, pelvic heaviness, and bloating, and feels as though she may have her menses. A transvaginal ultrasound shows endometrial thickness of 12 mm. An endometrial biopsy is performed and confirms endometrial adenocarcinoma. Endometrial cancer is the most common gynecologic malignancy and the fourth most common malignancy in women in the US
Diagnosis: Endometrial biopsy is the gold standard definitive diagnostic test
TX: Usually total hysterectomy and bilateral salpingo-oophorectomy, pelvic radiation therapy with or without chemotherapy for stage II or III cancer 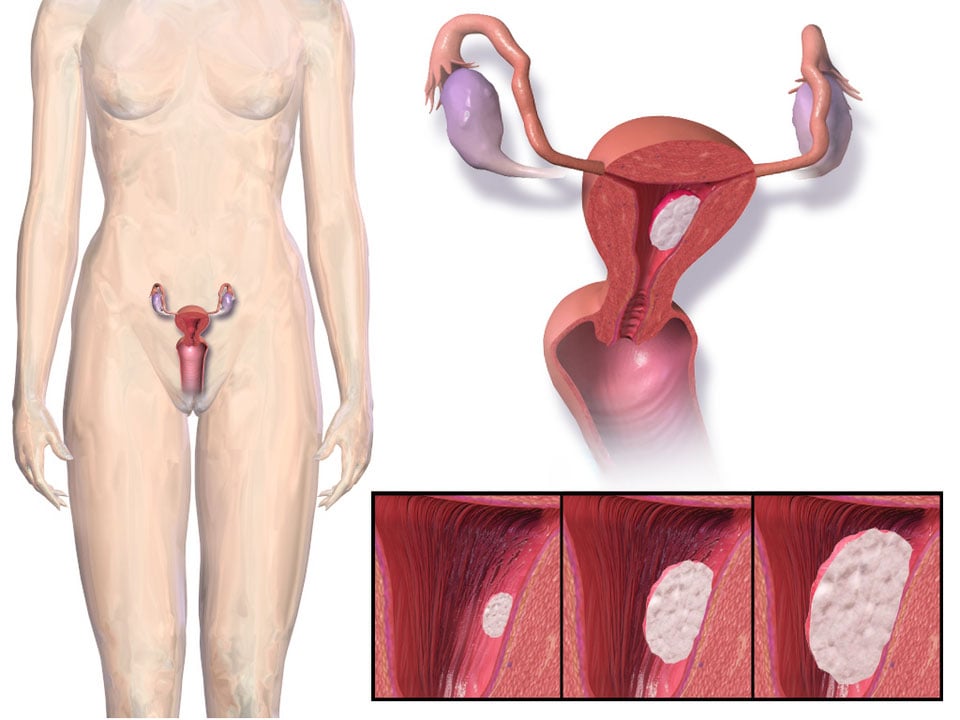 Endometrial cancer involving the uterine lining. Illustration by Blausen Medical Communications, Inc. via Wikimedia Commons, CC BY 3.0. |
| Vaginal and Vulvar Cancer | Patient will present as → a 65-year-old African American woman, gravida 4, para 4, with a smoking history and past HPV infection, presents with 3 months of postmenopausal vaginal bleeding, pelvic pain, and dyspareunia. She states that the bleeding is usually light and intermittent but has recently increased in frequency and volume. She hasn’t had a Pap smear in over a decade. On examination, a 2cm firm, irregular mass is found on the anterior vaginal wall. Biopsy reveals poorly differentiated squamous cell carcinoma, and the CT scan indicates local invasion into the bladder wall. (vaginal neoplasms)
Patient will present as → a 50-year-old female with vaginal itching and irritation, red/white ulcerative crusted lesions on the vulva (vulvar cancer) Vaginal Cancer
TX: with radiation therapy  Stage III vaginal cancer with spread into the pelvic wall and/or regional lymph nodes. Illustration by Cancer Research UK via Wikimedia Commons, CC BY-SA 4.0. Patient will present as → a 50-year-old female with vaginal itching, and irritation, red/white ulcerative crusted lesions on the vulva Vulvar Cancer
DX: Application of acetic acid or staining with toluidine blue may help direct optimal biopsy location TX: Vulvectomy and lymph node dissection Paget’s – pruritic red lesions TX: Local resection 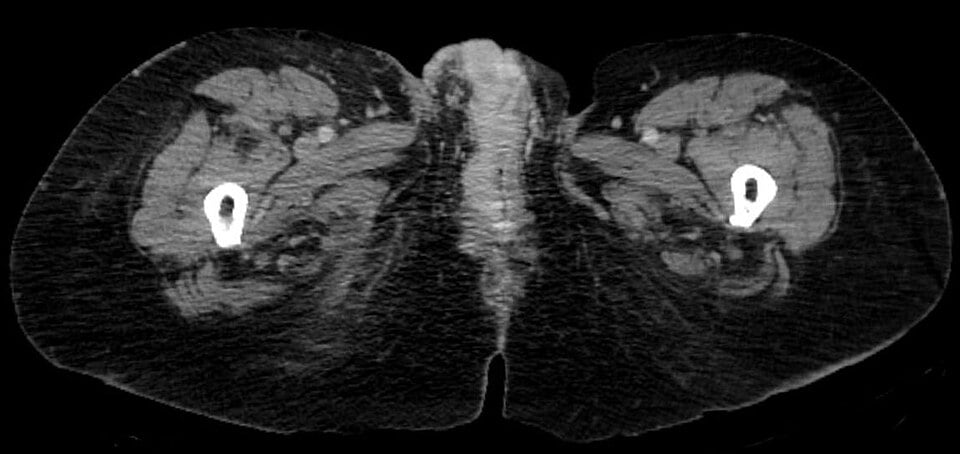 Right-sided vulvar carcinoma on axial CT imaging. Image by Hellerhoff via Wikimedia Commons, CC BY-SA 3.0. |
{kind=link}
{kind=link}