If you are like most PA students, you spend the lion's share of your time obsessed with the “Content” side of the NCCPA PANCE Blueprint.
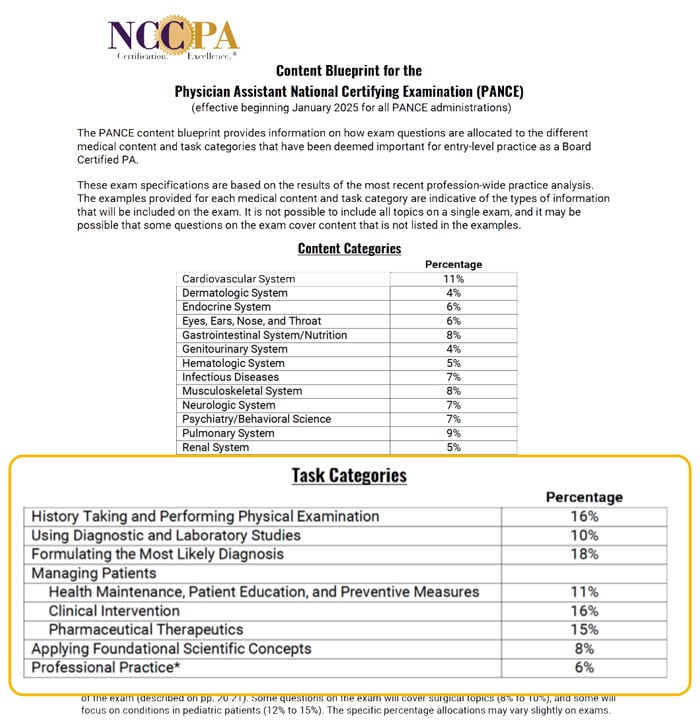
You have likely memorized the percentages of the heavy hitters like Cardiovascular (11%), Pulmonary (9%), Gastrointestinal (8%), and Musculoskeletal (8%). You have been told that to pass, you need to master these high-yield organ systems.
But while you were busy memorizing the valvular disorders and the difference between Ulcerative Colitis and Crohn’s, you probably ignored the other half of the grid: The Task Categories. 👈 (click that link to see the official NCCPA PANCE task categories).
Every PANCE question has two dimensions:
- The Content: What organ system it belongs to (these are the 14 organ systems you know and love)
- The Task: The specific cognitive skill it is testing (the 9 task categories everyone ignores)
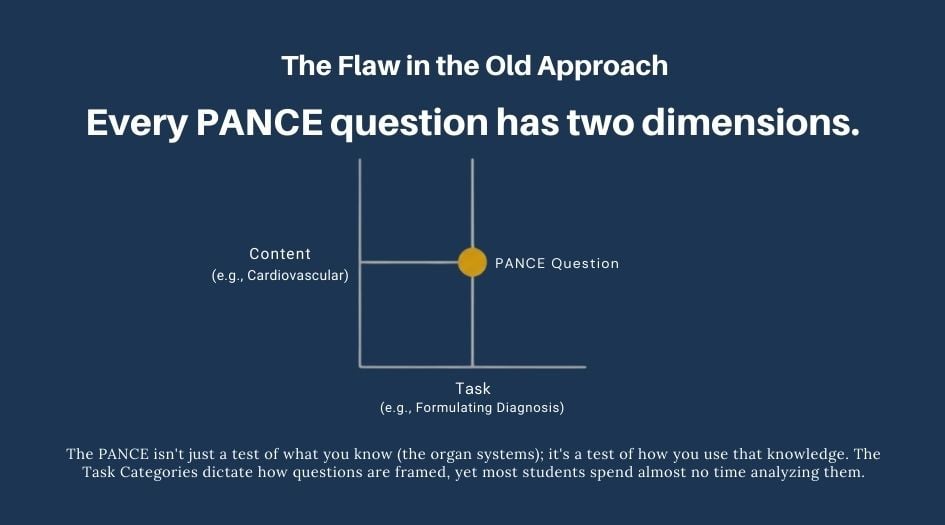
The PANCE isn’t just a test of what you know (the organ systems); it is a test of how you use that knowledge. The Task Categories dictate how questions are asked, yet most students (and many instructors) spend almost zero time analyzing them.
Here is the truth about why the exam is structured the way it is and how you can use this “hidden blueprint” to study smarter.
The Method Behind the Madness: The Clinical Loop
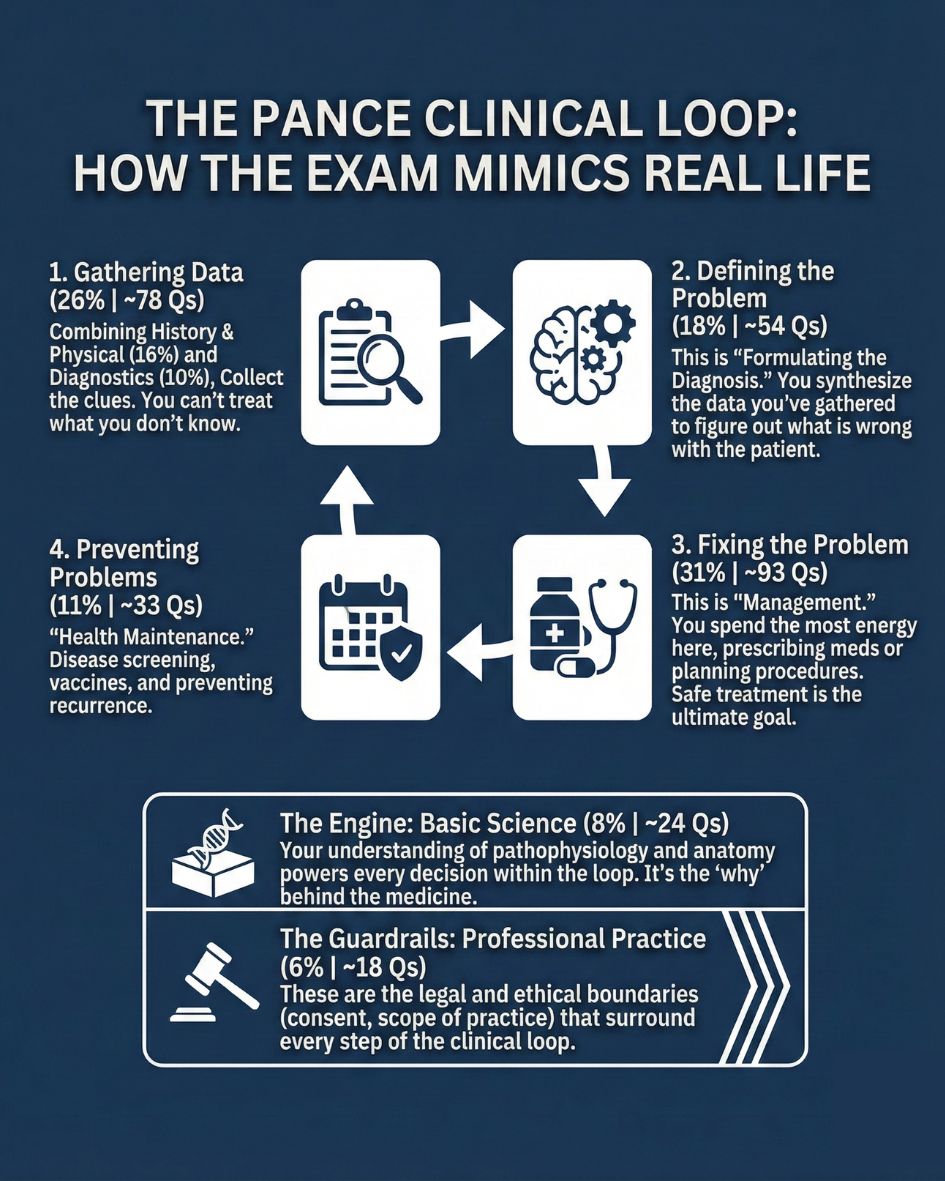
The percentages assigned to the Task Categories are not arbitrary. The exam mirrors the workflow of a real-life clinician, focusing heavily on the “Clinical Loop”: (1) Gathering Data, (2) Defining the Problem, (3) Fixing It, and (4) Preventing It.
However, this loop doesn’t function in a vacuum. Think of the Clinical Loop as the "Software" you run every day. But software can't run without an Operating System.
- The Engine (8%): You cannot run the loop without the Foundational Scientific Concepts (Anatomy/Pathophysiology) that drive your decisions.
- The Guardrails (6%): You must perform every step of the loop within the legal and ethical boundaries of Professional Practice.
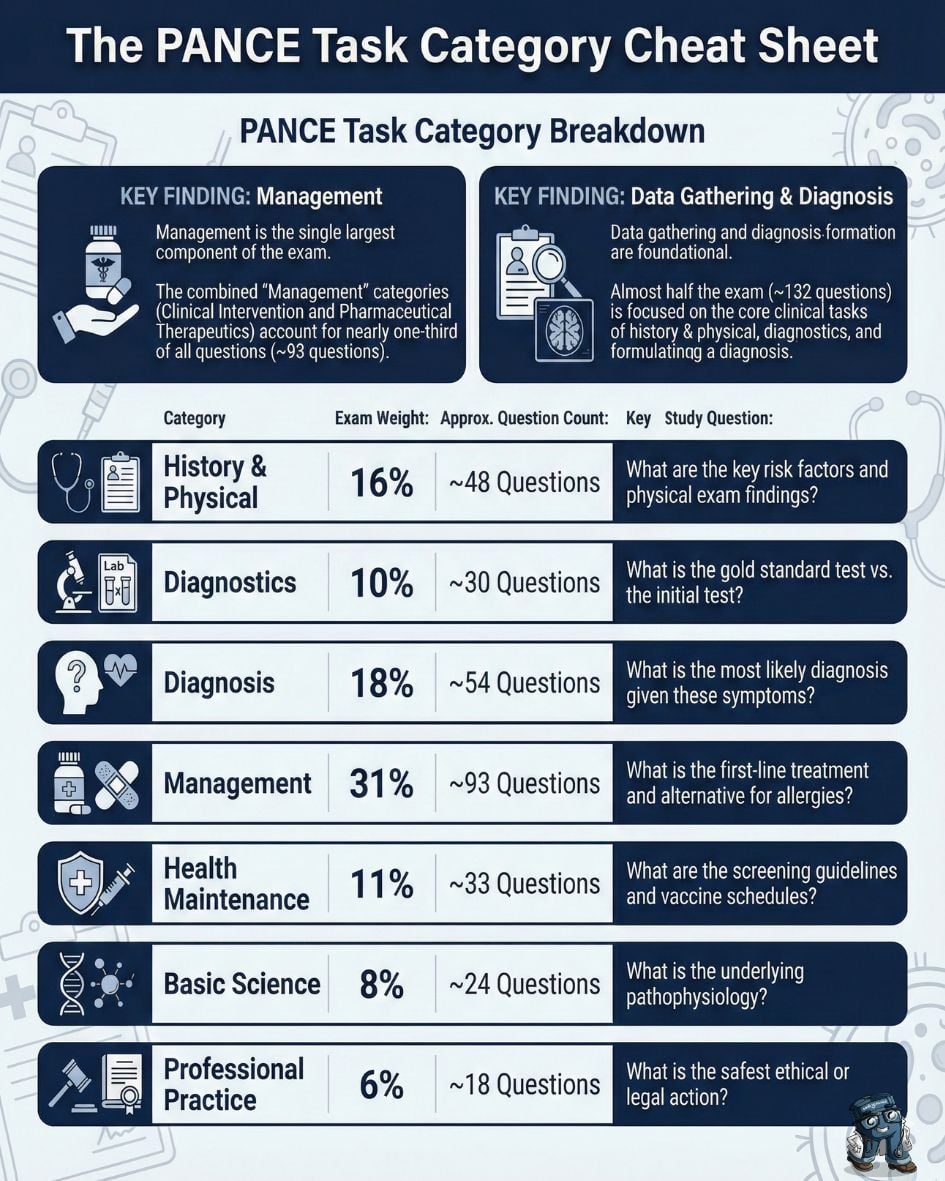
Here is how the PANCE blueprint's task categories fit together:
1. Gathering Data (26%)
(~78 Questions)
You cannot treat what you don’t know. The combination of History Taking and Performing Physical Examination (16%) and Using Diagnostic and Laboratory Studies (10%) makes up over a quarter of the exam. This reflects the reality that a PA’s first job is accurate data collection.
History Taking & Performing Physical Examination (16%)
(~48 Questions)
This category tests your knowledge of pertinent historical information, risk factors, and significant physical examination findings. It’s not just about “what is the disease?” but “how do you find the disease?”
What a Question Looks Like:
A 45-year-old male presents with a sudden onset of severe pain in his right big toe. He admits to heavy alcohol consumption the previous night. On physical examination, the joint is swollen, erythematous, and exquisitely tender to touch. This patient has a history of similar flares over the last 10 years.
The presence of which of the following physical exam findings would most strongly support a diagnosis of chronic tophaceous gout?
- Heberden’s nodes
- Ulnar deviation
- Hard, painless nodules on the helix of the ear
- Malar rash
The Clue: Notice the question didn't ask "What is the diagnosis?" (Gout). It asked you to hunt for a specific physical sign of chronicity.
Using Diagnostic and Laboratory Studies (10%)
(~30 Questions)
This section focuses on indications, risks, and cost-effective use of diagnostics. It also covers interpreting results to differentiate between diagnoses.
What a Question Looks Like:
A 24-year-old female presents with fatigue and heavy menses. A CBC reveals a microcytic, hypochromic anemia. You suspect iron deficiency anemia.
Which of the following laboratory profiles would best confirm this diagnosis?
- Low serum iron, low ferritin, high TIBC
- Low serum iron, high ferritin, low TIBC
- High serum iron, high ferritin, normal TIBC
- Normal serum iron, normal ferritin, normal TIBC
The Clue: Iron deficiency is characterized by low iron stores (ferritin) and increased binding capacity (TIBC).
2. Defining the Problem (18%)
(~54 Questions)
Formulating the Most Likely Diagnosis (18%)
(~54 Questions)
This is the highest-weighted individual category outside of management. These questions ask you to synthesize the history, physical exam, and labs to select the correct diagnosis from a list of differentials.
What a Question Looks Like:
A 65-year-old male with a history of smoking presents with painless hematuria. He denies dysuria or flank pain. A CT urogram reveals a solid mass in the bladder.
What is the most likely diagnosis?
- Renal cell carcinoma
- Bladder calculi
- Urothelial (transitional cell) carcinoma
- Acute cystitis
The Clue: Painless hematuria in a smoker is bladder cancer until proven otherwise; Urothelial carcinoma is the most common type.
3. Fixing the Problem (31%)
(~93 Questions)
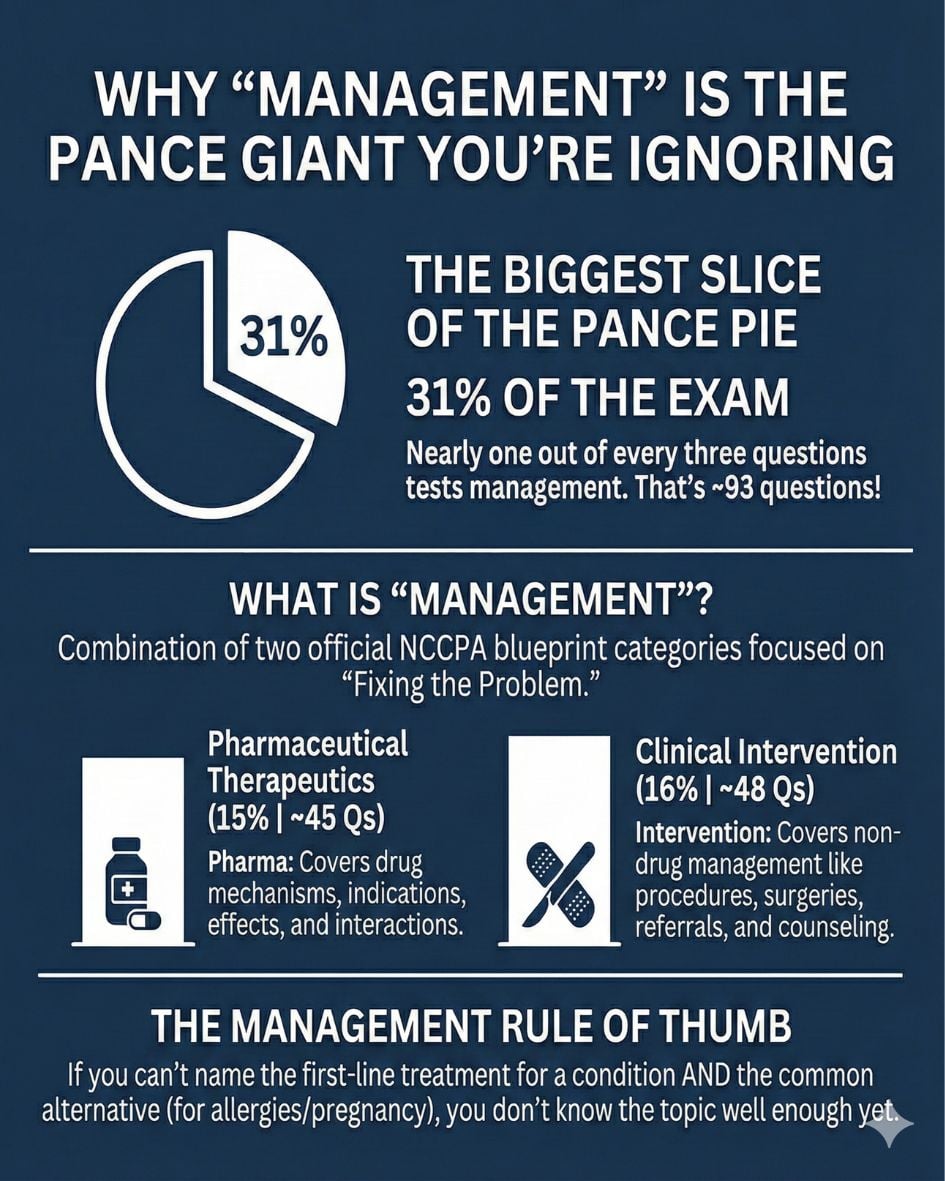
Identifying the disease is useless if you can’t treat it. Clinical Intervention (16%) and Pharmaceutical Therapeutics (15%) combined form the largest functional area of the test—nearly 100 questions! This signals that safe treatment is the ultimate goal of certification.
Clinical Intervention (16%)
(~48 Questions)
The Rule: If it involves a knife, a tube, a referral, or a conversation—it is Intervention.
This includes procedures, surgeries, referrals, and counseling on lifestyle modifications or discharge planning.
What a Question Looks Like:
A 22-year-old male presents to the ED with a primary spontaneous pneumothorax estimated at 10% of the hemithorax volume. He is stable and asymptomatic.
What is the most appropriate initial clinical intervention?
- Needle decompression
- Tube thoracostomy
- Observation and supplemental oxygen
- Video-assisted thoracoscopic surgery (VATS)
The Clue: Small, stable primary pneumothoraces are typically managed with observation. You are choosing the safest step, not just the most aggressive one.
Pharmaceutical Therapeutics (15%)
(~45 Questions)
The Rule: If it involves a pill or an IV—it is Pharma.
This covers the mechanism of action, indications, contraindications, drug interactions, and adverse effects.
What a Question Looks Like:
You are prescribing an ACE inhibitor for a patient with heart failure. Which of the following is a known adverse effect that would necessitate discontinuing the medication?
- Hypokalemia
- Angioedema
- Dry mouth
- Bradycardia
The Clue: Angioedema is a life-threatening reaction to ACE inhibitors.
4. Preventing Problems (11%)
(~33 Questions)
Health Maintenance, Patient Education, and Preventative Measures (11%)
Focus on USPSTF screening guidelines, vaccination schedules, and identifying risk factors for disease prevention.
What a Question Looks Like:
According to current guidelines, at what age should a patient with average risk begin screening colonoscopy for colorectal cancer?
- 40 years old
- 45 years old
- 50 years old
- 55 years old
The Clue: The USPSTF lowered the screening age to 45 in recent updates.
5. The Engine: Foundational Scientific Concepts (8%)
(~24 Questions)
You might be surprised to see that Applying Foundational Scientific Concepts accounts for only 8% of the exam content. But don’t be fooled by the low number—this category is the engine that powers the Clinical Loop.
You cannot “Define the Problem” (Step 2) or “Fix the Problem” (Step 3) if you don’t understand the machinery under the hood.
What a Question Looks Like:
Which of the following describes the underlying pathophysiologic mechanism of Graves’ disease?
- Destruction of thyroid follicles by autoimmune antibodies
- Stimulation of TSH receptors by thyroid-stimulating immunoglobulins
- Iodine deficiency leading to TSH hypersecretion
- Benign functioning adenoma of the pituitary gland
The Clue: Graves’ disease is caused by antibodies that stimulate the TSH receptor, leading to hyperthyroidism.
6. The Guardrails: Professional Practice (6%)
(~18 Questions)
There is one final category that wraps around the entire Clinical Loop: Professional Practice.
While the Clinical Loop dictates what you do (diagnose, treat, prescribe), Professional Practice dictates how you are allowed to do it. These are the legal and ethical guardrails that surround every single patient interaction.
What a Question Looks Like:
A competent 55-year-old male with active GI bleeding refuses a blood transfusion due to religious beliefs. You have explained the risks of death extensively.
What is the most appropriate ethical action?
- Honor the patient’s refusal and document the discussion.
- Administer the transfusion due to the life-threatening nature of the condition.
- Contact the hospital’s risk management department for immediate legal authorization to treat.
- Request a psychiatric consultation to assess the patient’s capacity.
The Clue: Competent patients have the right to refuse treatment, even if life-sustaining.
The "15-Minute Visit" Analogy
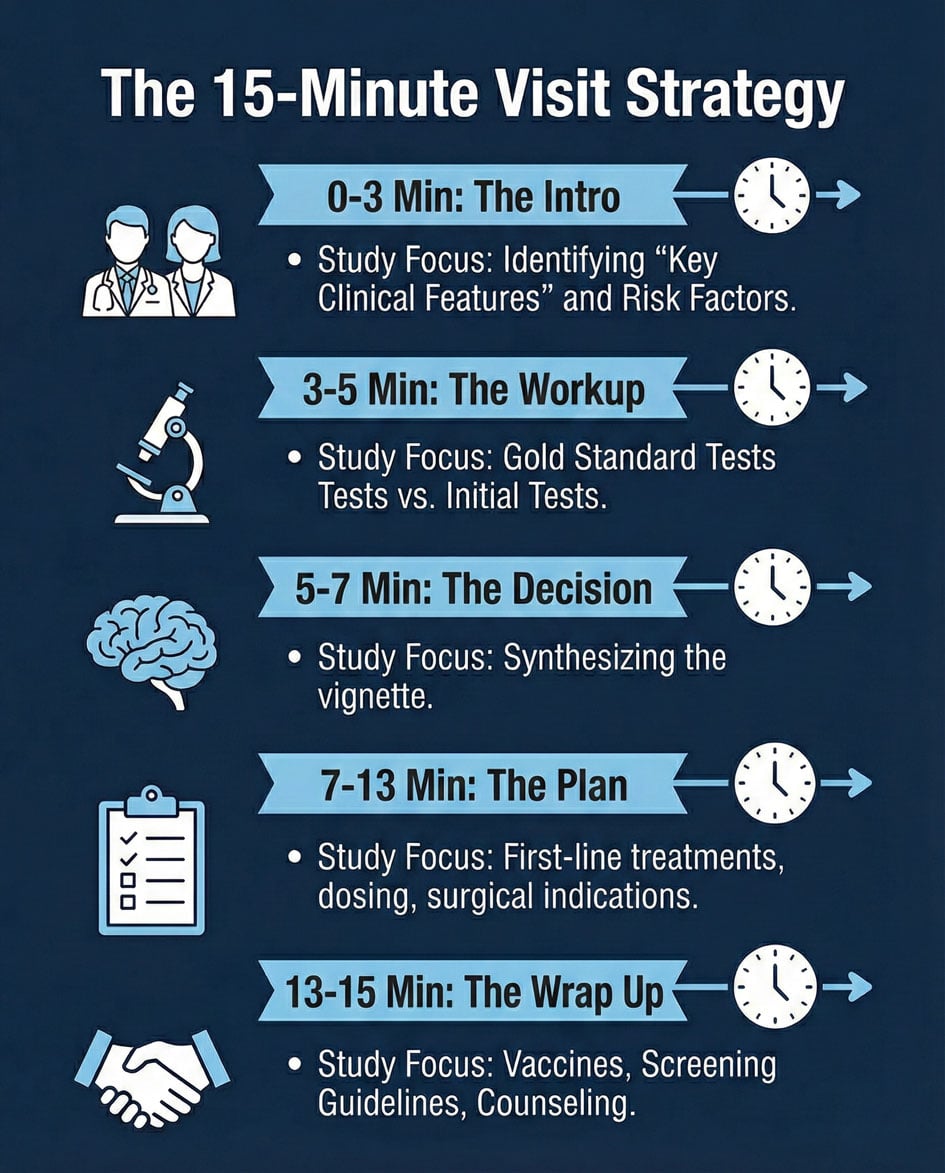
To understand the weighting, visualize a standard 15-minute patient appointment. The exam percentages almost perfectly track the energy you spend during that visit:
1. The Intro (16%): You start by talking to the patient and examining them (History/Physical).
2. The Workup (10%): You decide if you need blood work or imaging (Diagnostics).
3. The Decision (18%): You synthesize that data to figure out what is wrong (Diagnosis).
4. The Plan (31%): You spend the bulk of your mental energy prescribing meds or performing a procedure (Pharma/Intervention).
5. The Wrap-Up (11%): You finish by explaining how to stay healthy or prevent recurrence (Health Maintenance).
Wait, that only adds up to 86%?
The remaining 14% (Basic Science & Professional Practice) are the Operating System. They are running in the background during every single minute of that visit. You are constantly accessing anatomy (science) and ensuring you have consent (Professional Practice) throughout the visit.
The 7 Faces of One Disease
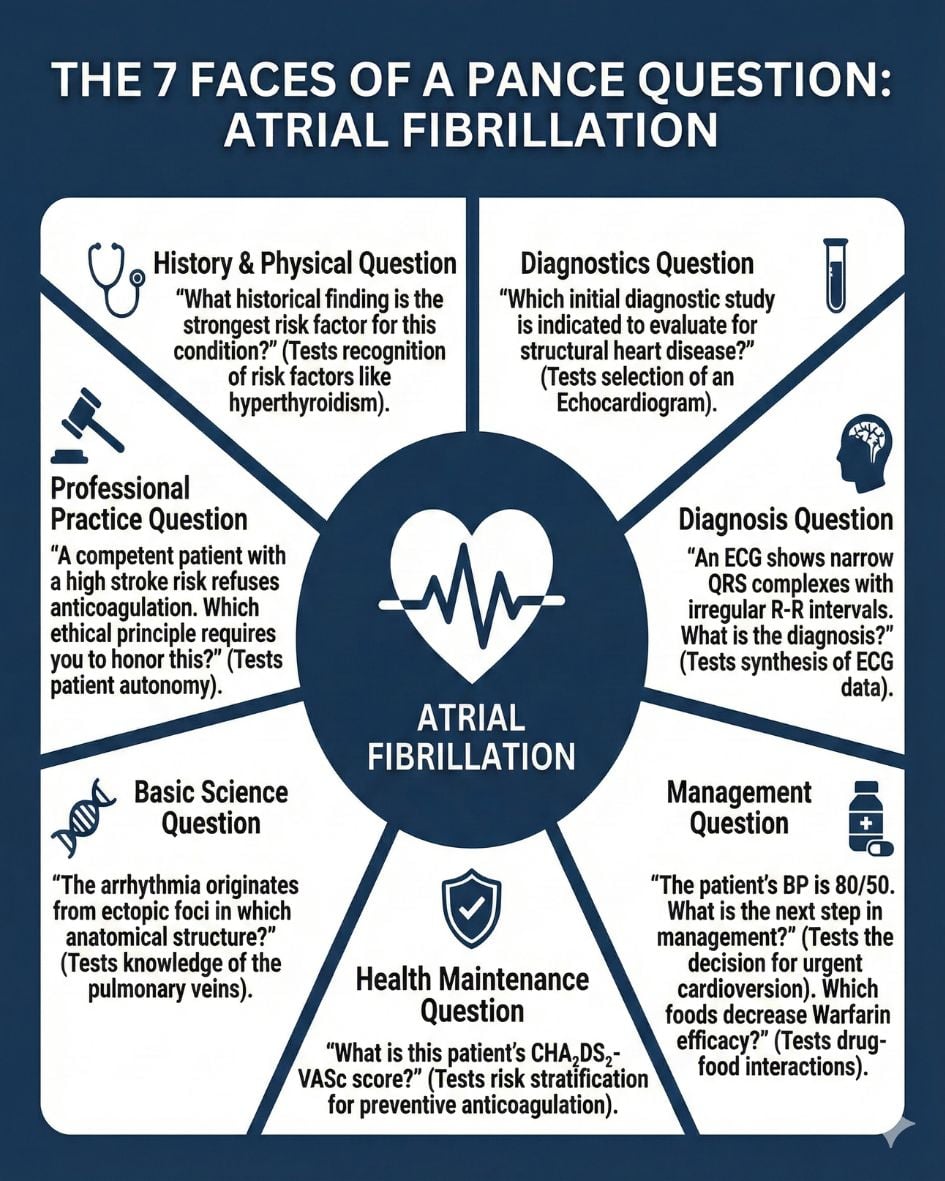
To understand how this affects your studying, consider how one medical topic (e.g., Atrial Fibrillation) can be asked about in 7 different ways depending on the Task Category.
- History Taking (16%): “What historical finding is the strongest risk factor for this condition?”
- The Pivot: You are a Historian. You aren't treating; you are looking for causes (e.g., hyperthyroidism).
- Diagnostic Studies (10%): “Which initial diagnostic study is indicated to evaluate for structural heart disease?”
- The Pivot: You are an Investigator. You are choosing the tool (e.g., Echo).
- Formulating Diagnosis (18%): “ECG shows narrow QRS complexes with variable R-R intervals. What is the diagnosis?”
- The Pivot: You are a Detective. You are naming the beast.
- Health Maintenance (11%): “What is this patient’s CHA2DS2-VASc score?”
- The Pivot: You are a Protector. You are stratifying risk for the future.
- Clinical Intervention (16%): “BP is 80/50… What is the next step?”
- The Pivot: You are a First Responder. The name of the disease matters less than the stability (e.g., Cardioversion).
- Pharmaceutical Therapeutics (15%): “Which foods decrease the efficacy of Warfarin?”
- The Pivot: You are a Pharmacist. You are managing interactions.
- Foundational Scientific Concepts (8%): “The arrhythmia originates from ectopic foci in which anatomical structure?”
- The Pivot: You are a Scientist. You are recalling anatomy (e.g., pulmonary veins).
How to Study Smarter, Not Harder
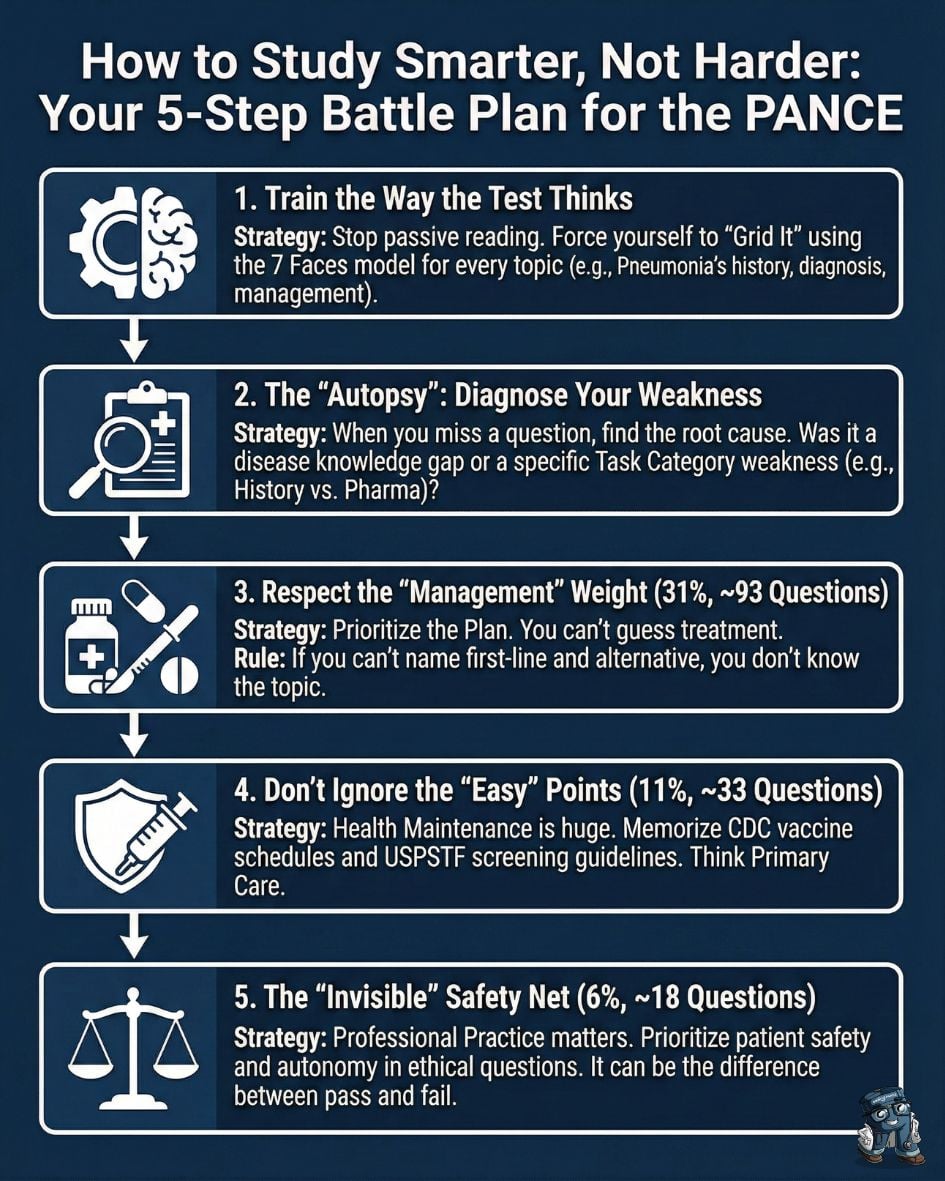
Now that you see the matrix, you can stop passively reading and start actively training.
1. Train the Way the Test Thinks
Most students study vertically (by organ system), but the test asks questions horizontally (by task). When you review a topic, force yourself to “Grid It.” Don’t just read the chapter on Pneumonia. Stop and explicitly ask yourself the seven questions from the 7 Faces model.
2. The “Autopsy”: Diagnose Your Weakness
When you miss a practice question, perform an “autopsy.”
- Scenario: You missed a Heart Failure question because you picked a Calcium Channel Blocker instead of an ACE Inhibitor.
- Diagnosis: This is a Pharmaceutical Therapeutics (15%) weakness. You knew the disease, but you failed the task.
3. Respect the “Management” Weight (~93 Questions)
Clinical Intervention and Pharma make up 31% of the exam. If you are crunched for time, prioritize the Plan. You can often reason your way to a diagnosis, but you cannot “guess” a specific drug mechanism or surgical indication.
4. Don’t Ignore the “Easy” Points (~33 Questions)
Health Maintenance (11%) accounts for roughly 33 questions. That is more than the entire Pulmonary system (9%). Memorize the CDC Vaccine Schedule and USPSTF Cancer Screening guidelines. This is “free money” on the table.
5. The “Invisible” Safety Net (~18 Questions)
Finally, do not forget Professional Practice (6%). These 18 questions often determine whether a borderline student passes or fails.
The Strategy: You cannot “cram” ethics, but you can learn the principles. When in doubt on a non-medical question, the answer is almost always the one that prioritizes patient safety and patient autonomy over provider comfort or institutional policy.
By aligning your study habits with the NCCPA PANCE blueprint percentages, you aren’t just working hard — you’re working smart.
Stop Guessing. Start Training.
The volume of medical knowledge required for the PANCE can feel paralyzing. There is always "one more disease" to learn. But while you can’t memorize every line of PANCE PREP PEARLS, you can master the Task Categories.
When you understand the structure of the question, the content becomes less intimidating.
- A "History" question isn't asking for the cure; it's asking for the clue.
- A "Therapeutics" question isn't asking for the pathology; it's asking for the pill.
This shift in perspective is often the difference between a borderline score and a confident pass.
Build Your Clinical Reflexes
At Smarty PANCE, we design our questions to reflect this exact level of complexity. We don't just ask for simple recall; we challenge you across the entire Clinical Loop. Our content ensures you aren't just memorizing diseases, but practicing the specific skills—from diagnostics to management—that you need to pass on exam day.
👉 Start your targeted training plan with Smarty PANCE today.



{kind=link}