Ménière's disease, labyrinthitis, vestibular neuritis, benign paroxysmal positional vertigo (BPPV), and acoustic neuroma are all causes of vertigo and are included on the NCCPA PANCE/PANRE EENT blueprint and family medicine rotation exam blueprints.
It is important to be able to differentiate quickly between these five causes of vertigo. They are common exam questions with significant overlap that exam writers leverage while creating high-quality clinical vignettes.
Let's take a quick look at how patient presentations will differ among these conditions and identify the key differences so that you can quickly make the correct diagnosis.
How to Differentiate Between Meniere's Disease, Labyrinthitis, Vestibular Neuritis, and Acoustic Neuroma
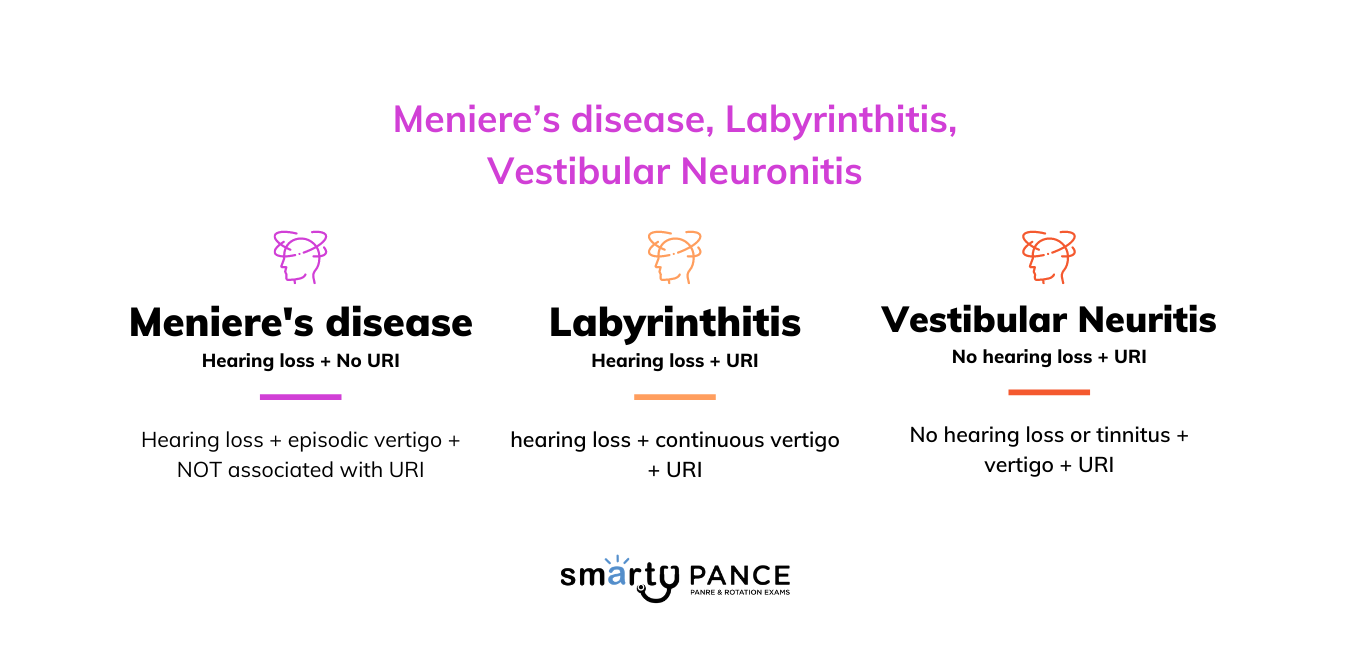
- Labyrinthitis (affects entire labyrinth and vestibulocochlear nerve) = hearing loss + continuous vertigo + URI
- Vestibular neuritis (affects vestibular nerve) = NO hearing loss or tinnitus + vertigo + URI
- Meniere's disease = hearing loss + episodic vertigo + NOT associated with URI
- Benign paroxysmal positional vertigo = No hearing loss or tinnitus + episodic vertigo with position changes
- Acoustic neuroma = Unilateral hearing loss, insidious onset vertigo, and ataxia +/- facial numbness
| Disease | Cause | Characteristics | Symptoms | Diagnostic Test | Treatment |
| Benign positional vertigo | Otoconia (calcium carbonate crystals) dislodged from otolith organs, moving into semicircular canals | Changes with position | Vertigo without hearing loss, tinnitus, or ataxia | MRI of the internal auditory canal | Diagnosis: Dix-Hallpike maneuver
Treatment: Epley maneuver Meclizine |
| Vestibular neuritis | Viral infection affecting the vestibular nerve but sparing the cochlear branch | Vertigo without position changes | Vertigo but no hearing loss or tinnitus (inflammation of vestibular portion of CN VIII) | Meclizine | |
| Labyrinthitis | Often viral infection, sometimes bacterial
Labyrinthitis involves inflammation of the labyrinth. It affects both the vestibular nerve (balance) and the cochlear branch (which transmits hearing information). It can cause a feeling of spinning (vertigo) and hearing loss. |
Acute, self-resolving episode | Continuous Vertigo
Hearing loss Tinnitus Self-limited |
Meclizine + steroids | |
| Meniere's disease | Unknown, but involves fluid buildup in the inner ear
Not associated with URI |
Chronic remitting and relapsing episodes | Episodic Vertigo
Hearing loss Tinnitus and chronic remitting and relapsing manner |
Diuretics
Salt restriction Unilateral CN VIII ablation (severe cases) |
|
| Acoustic neuroma | Benign tumor on the vestibulocochlear nerve (CN VIII) | Ataxia
Neurofibromatosis type II MRI findings Facial numbness |
Vertigo
Unilateral hearing loss Tinnitus AND ataxia |
Surgical intervention |
Question 1 |
Meniere's disease Hint: Meniere's disease involves episodic vertigo, hearing loss, tinnitus, and aural fullness. | |
Vestibular neuritis Hint: Vestibular neuritis presents with prolonged vertigo but not triggered by head movements, and without hearing loss. | |
Labyrinthitis Hint: Labyrinthitis includes vertigo and hearing loss, not solely provoked by position changes. | |
Benign paroxysmal positional vertigo | |
Acoustic neuroma Hint: Acoustic neuroma typically presents with progressive unilateral hearing loss and tinnitus, not episodic positional vertigo. |
Question 2 |
Benign paroxysmal positional vertigo Hint: BPPV causes brief episodes of vertigo related to head position changes. | |
Vestibular neuritis | |
Labyrinthitis Hint: Labyrinthitis also presents with auditory symptoms like hearing loss. | |
Meniere's disease Hint: Meniere's disease involves episodic vertigo, hearing loss, tinnitus, and aural fullness. | |
Acoustic neuroma Hint: Acoustic neuroma usually presents with unilateral hearing loss and tinnitus, not acute vertigo. |
Question 3 |
Benign paroxysmal positional vertigo Hint: BPPV is characterized by brief, positionally triggered episodes of vertigo without hearing loss. | |
Vestibular neuritis Hint: Vestibular neuritis presents with vertigo but without hearing loss or tinnitus. | |
Labyrinthitis | |
Meniere's disease Hint: Meniere's disease involves episodic vertigo, not continuous, along with fluctuating hearing loss. | |
Acoustic neuroma Hint: Acoustic neuroma presents with progressive hearing loss and tinnitus, typically without acute vertigo episodes. |
Question 4 |
Benign paroxysmal positional vertigo Hint: BPPV involves short-lived vertigo episodes triggered by head movements, without auditory symptoms. | |
Vestibular neuritis Hint: Vestibular neuritis is marked by a single prolonged episode of vertigo without hearing loss. | |
Labyrinthitis Hint: Labyrinthitis presents with continuous vertigo and hearing loss, typically following an infection. | |
Meniere's disease | |
Acoustic neuroma Hint: Acoustic neuroma involves progressive unilateral hearing loss and tinnitus but not episodic vertigo. |
Question 5 |
Acoustic neuroma | |
Benign paroxysmal positional vertigo (BPPV) Hint: BPPV causes episodic vertigo without hearing loss or tinnitus. | |
Labyrinthitis Hint: Labyrinthitis includes vertigo and hearing loss but is not associated with a mass on imaging. | |
Meniere's disease Hint: Meniere's disease involves episodic vertigo and hearing loss but not due to a cerebellopontine angle mass. | |
Vestibular neuritis Hint: Vestibular neuritis presents with acute vertigo but no hearing loss. |
|
List |


