 Lecture
Lecture
Patient will present as → a 32-year-old male with complaints of recurrent, episodic vertigo lasting up to 8 hours per episode for the past 3 months. The attacks generally last less than half an hour and are associated with decreased low-frequency hearing in the left ear along with nonpulsatile tinnitus in the ipsilateral ear. You obtain an audiogram that shows a low-frequency hearing loss in the left ear only.

To watch this and all of Joe Gilboy PA-C's video lessons you must be a member. Members can log in here or join now.
Ménière syndrome is a disorder of the endolymphatic compartment with the classic triad of episodic vertigo, unilateral low-frequency sensorineural hearing loss, and tinnitus.
Vestibular neuritis is an inflammation of the vestibular nerve. Vestibular neuritis presents with continuous vertigo, nausea, and vomiting, but not hearing loss or tinnitus. It is related to viral URIs, and develops over several hours, with symptoms worse in the first day, with gradual recovery over several days. The symptoms of vestibular neuritis are the same as labyrinthitis minus tinnitus and/or hearing loss.
Ménière syndrome is a disorder of the endolymphatic compartment with the classic triad of episodic vertigo, unilateral low-frequency sensorineural hearing loss, and tinnitus. Labyrinthitis is similar to Meniere’s disease except that labyrinthitis causes continuous symptoms (vs. the episodic symptoms of Meniere’s disease).
Benign paroxysmal positional vertigo (BPPV) is generally thought to be due to debris that has collected within a part of the inner ear. BPPV occurs with changes in position, especially rapid movements of the head. Nausea may occur, but vomiting is not significant. It causes episodic vertigo without hearing loss.
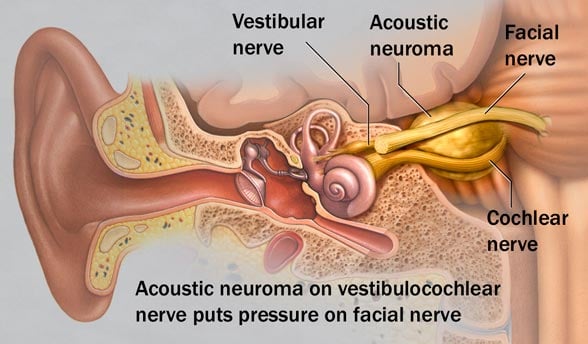
Acoustic neuroma is a benign tumor of the Schwann cells (the cells which produce myelin sheath). Patient will present with an insidious unilateral hearing loss, tinnitus, headache, facial numbness, continuous disequilibrium (unsteadiness), +/- vertigo.
{kind=link}

"To differentiate labyrinthitis from Meniere's disease on your exam look for tinnitus and episodic symptoms. Labyrinthitis is similar to Meniere's disease except that labyrinthitis causes continuous symptoms and has the combination of vertigo + hearing loss and (although it can) is less likely to present with tinnitus on exam questions."
Pt will often present with episodic peripheral vertigo lasting 1-8 hours with nystagmus, nausea, and vomiting.
Clinical diagnosis (AAO-HNS criteria): ≥2 definitive vertigo episodes (20 min–24 h) + audiometrically documented SNHL + ipsilateral tinnitus or aural fullness + no other diagnosis
- The diagnosis of Meniere disease, made clinically, is primarily one of exclusion. Similar symptoms can result from vestibular migraine, viral labyrinthitis or neuritis, a cerebellopontine angle tumor (eg, acoustic neuroma), or a brain stem stroke
- Although bilateral Meniere disease can occur, bilateral symptoms increase the likelihood of an alternate diagnosis (eg, vestibular migraine)
- Patients with suggestive symptoms should have an audiogram and an MRI (with gadolinium enhancement) of the CNS with attention to the internal auditory canals to exclude other causes
- An audiogram typically shows a low-frequency sensorineural hearing loss in the affected ear that fluctuates between tests
- The Rinne test and the Weber test may also indicate sensorineural hearing loss
Lifestyle modifications (first-line): low-sodium diet (<1,500–2,000 mg/day), reduce caffeine, alcohol, stress
- Diuretics: hydrochlorothiazide/triamterene or acetazolamide — reduce endolymph production
- Betahistine: improves cochlear blood flow; widely used in Europe (limited FDA approval)
- Acute attack: vestibular suppressants (meclizine, diazepam), antiemetics
- Intratympanic gentamicin: ablates vestibular function in refractory cases; preserves hearing better than surgical approaches
- Intratympanic steroids: for acute hearing loss episodes; less effective for vertigo
- Endolymphatic sac surgery or labyrinthectomy/vestibular neurectomy: for medically refractory severe cases
 Meniere’s Disease is a condition of the inner ear of unknown origin but characterized by excess endolymph in the vestibular and semicircular canals, causing increased fluid pressure in the inner ear; also known as endolymphatic hydrops. Symptoms usually begin between 30 to 60 years of age. Attacks are sudden and severe and may last hours or days.
Meniere’s Disease is a condition of the inner ear of unknown origin but characterized by excess endolymph in the vestibular and semicircular canals, causing increased fluid pressure in the inner ear; also known as endolymphatic hydrops. Symptoms usually begin between 30 to 60 years of age. Attacks are sudden and severe and may last hours or days.
| Meniere’s Disease | Play Video + Quiz |
| Vertigo | Play Video + Quiz |
| Thiazide diuretics | Play Video + Quiz |
Question 1 |
Acute labyrinthitis Hint: Acute labyrinthitis typically presents with an acute onset of continuous vertigo that lasts several days to a week and is associated with nausea and vomiting. It does not have any associated auditory or neurologic symptoms. | |
Positional vertigo Hint: Positional vertigo occurs following changes in head positioning with very brief, less than 1 minute, episodes. Nystagmus occurs following the position change. | |
Acoustic neuroma Hint: Acoustic neuroma typically presents with hearing loss and tinnitus. The neuroma grows slowly and central compensatory mechanisms can prevent or minimize the vertigo. Vertigo, when present, is continuous and not episodic. | |
Ménière's syndrome |
Question 2 |
Epley maneuver Hint: Epley maneuver is used to treat benign paroxysmal positional vertigo. | |
Diuretics and low-sodium diet | |
Broad-spectrum antibiotics and Ibuprofen Hint: Broad-spectrum antibiotics and ibuprofen are used to treat otitis media, not Meniere's disease. | |
Scopolamine transdermal patch Hint: A scopolamine patch is useful for treatment of a single episode, but not long-term management. |
Question 3 |
Meniere's syndrome | |
Labyrinthitis Hint: Labyrinthitis is an acute onset of continuous, usually severe vertigo lasting several days to a week, accompanied by hearing loss and tinnitus. | |
Benign paroxysmal positioning vertigo Hint: Benign paroxysmal positioning vertigo is a type of vertigo associated with changes in head position, often rolling over in bed. | |
Vestibular neuronitis Hint: Vestibular neuronitis is a paroxysmal, usually single attack of vertigo that occurs without accompanying impairment of auditory function and will persist for several days to weeks before clearing. |
|
List |