 Lecture
LecturePatient will present as → a 35-year-old male presents with the acute onset of severe, continuous vertigo (described as the room "spinning" around him), nausea, and vomiting that started yesterday. He reports a sudden decrease in hearing in his left ear accompanied by a constant "ringing" sound. He recalls having an upper respiratory infection last week. On examination, he exhibits horizontal nystagmus that decreases with visual fixation. Otoscopy is normal. A Weber test lateralizes to the right ear, and a Rinne test is positive bilaterally. He has difficulty walking and prefers to remain still.

To watch this and all of Joe Gilboy PA-C's video lessons you must be a member. Members can log in here or join now.
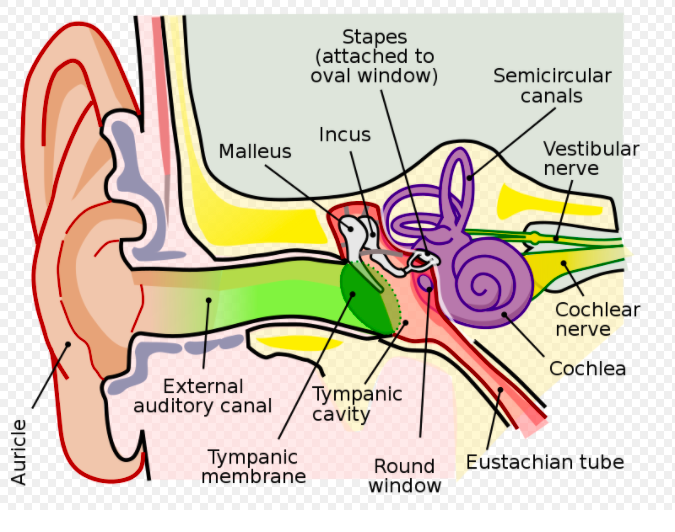
Labyrinthitis is an inflammatory condition of the inner ear labyrinth that affects both the vestibular (balance) and cochlear (hearing) components.
- The key diagnostic features are the acute and continuous onset of severe vertigo combined with unilateral sensorineural hearing loss and tinnitus
- Often preceded by a viral respiratory illness
- Affects the entire labyrinth, which includes the vestibulocochlear nerve - both branches - vestibular (balance) + cochlear (hearing)
- There is an absence of neurologic deficits
- Vertigo associated with labyrinthitis progressively improves over a few weeks, but the hearing loss may or may not resolve
{kind=link}

"Sometimes vestibular neuritis is used synonymously with viral labyrinthitis. However, vestibular neuronitis only presents with vertigo, while viral labyrinthitis is also accompanied by tinnitus, unilateral hearing loss, or both.Labyrinthitis is associated with CONTINUOUS vertigo along with unilateral hearing loss +/- tinnitus and is usually associated with an upper respiratory infection. This differentiates it from Meniere’s syndrome, which is EPISODIC and not typically associated with a viral infection."
Vestibular neuritis is an inflammation of the vestibular nerve. Vestibular neuritis presents with continuous vertigo, nausea and vomiting, but NOT hearing loss or tinnitus. It is related to viral URIs and develops over several hours, with symptoms worse on the first day, with gradual recovery over several days. The symptoms of vestibular neuritis are the same as labyrinthitis minus tinnitus and/or hearing loss.
- “Auditory function is preserved; when the symptoms and signs of vestibular neuritis are combined with unilateral hearing loss, the condition is called labyrinthitis.” – (UpToDate)
Ménière syndrome is a disorder of the endolymphatic compartment with the classic triad of episodic vertigo, unilateral low-frequency sensorineural hearing loss, and tinnitus. Labyrinthitis is similar to Meniere’s disease except that labyrinthitis causes continuous symptoms (vs. the episodic symptoms of Meniere’s disease).
Benign paroxysmal positional vertigo (BPPV) is generally thought to be due to debris that has collected within a part of the inner ear. BPPV occurs with changes in position, especially rapid movements of the head. Nausea may occur, but vomiting is not significant. It causes episodic vertigo without hearing loss.
Acoustic neuroma is a benign tumor of the Schwann cells (the cells that produce myelin sheath). A patient will present with an insidious unilateral hearing loss, tinnitus, headache, facial numbness, continuous disequilibrium (unsteadiness), +/- vertigo.
| Condition | Characteristics | Cause | Treatment |
| Labyrinthitis | Hearing loss, continuous vertigo, associated with upper respiratory infection (URI) | Often viral infection, sometimes bacterial
Affects the entire labyrinth and the vestibulocochlear nerve (affects the vestibular (balance) and cochlear (hearing) components) |
Supportive care, antiemetics for nausea, vestibular suppressants, corticosteroids for severe cases, and antibiotics if bacterial |
| Vestibular Neuritis | While it also presents with acute, severe vertigo, it is distinguished from labyrinthitis by the absence of hearing loss or tinnitus
Associated with URI |
Viral inflammation is limited to the vestibular nerve
Affects the vestibular (balance) nerve) |
Supportive care, antiemetics, vestibular rehabilitation, corticosteroids |
| Meniere's Disease | Hearing loss, episodic vertigo, not associated with URI | Unknown, but involves fluid buildup in the inner ear | Low-salt diet, diuretics, betahistine, invasive therapies for severe cases (e.g., intratympanic steroid injections, endolymphatic sac surgery) |
| Benign Paroxysmal Positional Vertigo (BPPV) | No hearing loss or tinnitus, episodic vertigo with position changes | Otoconia (calcium carbonate crystals) dislodged from otolith organs, moving into the semicircular canals | Epley maneuver or other canalith repositioning procedures, vestibular rehabilitation |
| Acoustic Neuroma | Unilateral hearing loss, insidious onset vertigo and ataxia, +/- facial numbness | Benign tumor on the vestibulocochlear nerve (CN VIII) | Observation for small, asymptomatic tumors, stereotactic radiosurgery, and surgical removal for larger or symptomatic tumors |
Labyrinthitis is a clinical diagnosis in the absence of neurologic deficits
- A key examination is the HINTS exam (Head Impulse, Nystagmus, Test of Skew), which helps differentiate between a peripheral cause (such as labyrinthitis or vestibular neuritis) and a central cause (like a stroke)
- In labyrinthitis, the exam typically shows a positive (abnormal) head impulse test, unidirectional horizontal nystagmus that suppresses with fixation, and a negative (normal) test of skew
- May have a positive Romberg test - fall to the side of the affected ear
- Rule out other etiologies with imaging, audiograms (will confirm the presence of sensorineural hearing loss), and TSH levels
- MRI is required for patients with acute, sustained vertigo whose examination is not entirely consistent with labyrinthitis, or in patients who are older (>60 years), or have a headache, any focal neurologic signs, or vascular risk factors
Vestibular suppressants (meclizine) and antiemetics (ondansetron) to limit symptoms in the first 24 to 48 hours
- A 10-day course of prednisone: 60 mg daily on days 1 through 5, 40 mg on day 6, 30 mg on day 7, 20 mg on day 8, 10 mg on day 9, and 5 mg on day 10
- Antibiotics are indicated with associated fever or signs of bacterial infection
Question 1 |
Vestibular neuronitis Hint: This condition typically presents with severe vertigo but without auditory symptoms such as hearing loss, making it less likely in this case. | |
Acute labyrinthitis | |
Benign paroxysmal positional vertigo (BPPV) Hint: BPPV causes brief episodes of vertigo related to changes in head position and does not involve hearing loss or middle ear fluid. | |
Orthostatic hypotension Hint: This refers to a significant drop in blood pressure upon standing, leading to dizziness or lightheadedness, but it would not explain the hearing loss or the presence of middle ear fluid. | |
Ménière's disease Hint: Characterized by episodic vertigo, fluctuating hearing loss, tinnitus, and a feeling of fullness in the ear, Ménière's disease is a chronic condition. The acute onset following an upper respiratory infection and the presence of fluid behind the eardrum are more indicative of labyrinthitis. |
Question 2 |
Meclizine, prochlorperazine, and oral hydration | |
Intravenous ceftriaxone Hint: Antibiotics are only indicated if there's suspicion of a bacterial cause, which is less common than viral labyrinthitis. | |
Tympanostomy tube placement Hint: This procedure is indicated for recurrent or chronic middle ear effusions, not acute labyrinthitis. | |
Oral prednisone Hint: Treatment with glucocorticoids during the acute period of vertigo was shown in at least one clinical trial to improve the recovery of peripheral vestibular function in patients with acute labyrinthitis. However, subsequent studies, albeit with many limitations, have not found a clear benefit of glucocorticoid therapy. | |
Epley maneuver Hint: This maneuver is used to treat Benign Paroxysmal Positional Vertigo (BPPV), a different condition involving displacement of otoconia. |
Question 3 |
Continuous vertigo Hint: Continuous vertigo is a hallmark symptom of labyrinthitis, resulting from the disturbance in the inner ear's balance mechanisms. Patients often describe a sensation of spinning or motion, which is consistent with labyrinthitis. | |
Sensorineural hearing loss Hint: Sensorineural hearing loss can occur in labyrinthitis due to inflammation affecting the cochlea. This type of hearing loss is a common finding in patients presenting with labyrinthitis. | |
Tinnitus Hint: Tinnitus, or ringing in the ears, is another symptom that can accompany labyrinthitis. It results from the cochlear involvement and is consistent with the disease's presentation. | |
Episodic vertigo with position changes | |
Nystagmus Hint: Nystagmus, involuntary eye movements, can be observed in patients with labyrinthitis as a result of the imbalance created by the inner ear's inflammation. It is a physical finding that supports the diagnosis of labyrinthitis. |
Question 4 |
Continuous vertigo lasting several days | |
Fluctuating hearing loss Hint: Both Labyrinthitis and Meniere's syndrome can present with hearing loss. However, fluctuating hearing loss is more characteristic of Meniere's syndrome | |
Positive Romberg test Hint: Fluctuating sensorineural hearing loss is characteristic of Meniere's syndrome. The buildup of endolymphatic fluid within the inner ear causes intermittent episodes of hearing changes. Although hearing loss can occasionally occur in labyrinthitis, it is not typically a fluctuating pattern. | |
Absence of nystagmus Hint: Nystagmus, involuntary eye movements, can occur in both Labyrinthitis and Meniere's syndrome due to the vestibular disturbance. Its absence does not reliably differentiate between the two conditions. | |
Presence of tinnitus Hint: Tinnitus (ringing or buzzing in the ears) is very common in both labyrinthitis and Meniere's syndrome. Its presence doesn't help differentiate the two. |
|
List |
References: Merck Manual · UpToDate