Patient will present as → a 68-year-old woman presents to the emergency department due to fatigue, malaise, and subjective fever. Her symptoms began approximately 1 week ago. Medical history is significant for small-cell lung cancer recently treated with doxorubicin plus cyclophosphamide and etoposide. Her temperature is 102°F (38.9°C) and blood pressure is 100/80 mmHg. A complete blood count with differential is remarkable for an absolute neutrophil count of 320 cells/mm3. She is admitted to the hospital and administered intravenous cefepime.
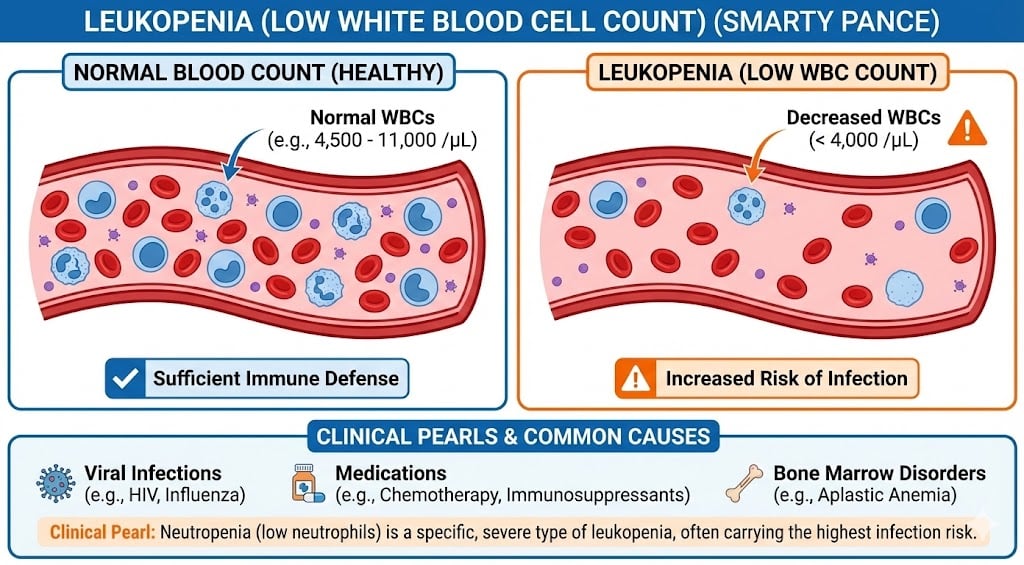
Leukopenia is a decrease in the total number of white blood cells (leukocytes) found in the blood, which places individuals at increased risk for infection
- Neutrophils are the first responders of immune cells
- Eosinophils fight bacteria and parasites, but also provoke allergy symptoms
- Basophils release histamine to mount a nonspecific immune response
- Monocytes clean up dead cells
- Lymphocytes (T cells and B cells) defend against specific invaders

"We can use the mnemonic 'Never Let Mamma Eat Beans' to remember the names of the different leukocytes."
Terminology:
- Leukopenia is a reduction in the circulating white blood cell (WBC) count. It is usually characterized by a reduced number of circulating neutrophils, although a reduced number of lymphocytes, monocytes, eosinophils, or basophils may also contribute. Thus, immune function can be decreased.
- Neutropenia, a subtype of leukopenia, refers to a decrease in the number of circulating neutrophil granulocytes, the most abundant white blood cells (40-70%). The terms leukopenia and neutropenia may occasionally be used interchangeably.
- Agranulocytosis is a complete absence of neutrophils - drugs that cause this include clozapine, propylthiouracil, penicillin G, methimazole, and dapsone.
- Lymphocytopenia is a decrease in the number of circulating lymphocytes. The most common cause of lymphopenia worldwide is protein-calorie malnutrition.
- Monocytopenia is a reduction in blood monocyte count. The major causes of this condition include use of myelotoxic drugs, acute infectious stress, aplastic anemia, hairy cell leukemia, and myeloid leukemia.
- Granulocytopenia is a reduced number of neutrophils, eosinophils, and basophils.
Low white cell count may be due to acute viral infections, such as a cold or influenza.
- Associated with chemotherapy, radiation therapy, myelofibrosis, aplastic anemia, stem cell transplant, bone marrow transplant, HIV, AIDS, and steroid use.
- Medical conditions such as systemic lupus erythematosus, Hodgkin's lymphoma, some types of cancer, etc.
- Medications such as clozapine, bupropion, minocycline, valproic acid, lamotrigine, metronidazole, immunosuppressive drugs, and interferons used to treat MS.
The absolute neutrophil count (ANC) is the number of neutrophils plus bands (does not include metamyelocytes and less mature forms). Mature neutrophils are also called polymorphonuclear cells (PMNs).
ANC = WBC (cells/microL) x percent (PMNs + bands) ÷ 100
Leukopenia can be identified with a complete blood count + blood smear
- Leukopenia is a reduced total WBC count of <4400 cells/microL
- Neutropenia is defined as an absolute neutrophil count (ANC) of less than <1500 cells/microL
- Agranulocytosis is defined as an ANC <200 cells/microL
- Monocytopenia is a reduction in blood monocyte count to < 500/microL
- Lymphocytopenia is a reduction in blood lymphocytes of < 1000/mcL
Additional tests
- Complete metabolic panel
- Blood cultures
- Urine culture
- Culture of sites concerning for infection
- Radiologic studies and CT scan
Treatment will be guided by the cause
- Discontinue causative agents
- Antibiotics in case of neutropenic fever
- Referral to hematology and/or specialized testing may be useful for patients in whom the cause for neutropenia has not been established by the initial evaluation
Question 1 |
Basopenia Hint: See C for explanation | |
Lymphocytopenia Hint: See C for explanation | |
Neutropenia | |
Monocytopenia Hint: See C for explanation |
Question 2 |
Broad-spectrum antibiotics | |
Immediate chemotherapy Hint: While chemotherapy is a cornerstone in the treatment of ALL, initiating or continuing chemotherapy in the setting of acute fever and profound neutropenia without first addressing the potential for infection could be harmful. | |
Granulocyte colony-stimulating factor (G-CSF) Hint: G-CSF is used to stimulate the production of neutrophils and may be part of the management to prevent future episodes of neutropenia, but it is not the first-line treatment for an acute febrile episode in a neutropenic patient. | |
Corticosteroids Hint: Corticosteroids are not the initial treatment of choice for febrile neutropenia and could potentially worsen the patient's immunocompromised state by further suppressing the immune system. | |
Observation and hydration Hint: While hydration is important for all patients, observation alone without the initiation of antibiotics in a febrile neutropenic patient is inappropriate due to the high risk of severe infections. |
Question 3 |
Hemoglobin electrophoresis Hint: Used to identify hemoglobinopathies, not directly useful for diagnosing the cause of leukopenia. | |
Bone marrow biopsy Hint: May be necessary for further evaluation but is not the first step.
| |
Direct Coombs test Hint: Used to diagnose autoimmune hemolytic anemia, not leukopenia. | |
Peripheral blood smear | |
Serum electrolyte panel Hint: Assesses electrolyte balance and kidney function, not specific for diagnosing the cause of leukopenia. |
|
List |
References: Merck Manual · UpToDate