| INFECTIOUS DISEASE | |
|
Flashcards ready when you areYou have opened several Quizlet sets recently. Loading this one only when needed helps prevent a temporary Quizlet limit.
|
|
| Atypical mycobacterial disease | Patient will present as → a 3-year-old with a firm, inflamed swelling in the right submandibular area. Initial medical management with intravenous antibiotics was ineffective. Fine needle aspiration of the lesion reveals acid-fast bacilli on Ziehl-Neelsen staining. Subsequent biopsy demonstrates a granulomatous reaction in keeping with a Mycobacterial infection. Specific questioning reveals no family history of tuberculosis, abscesses, or infections; there are no family pets, no exposure to birds, and no unpasteurized milk consumption. An initial chest x-ray was normal, and Mantoux testing was negative. Conventional anti-tuberculous therapy (Isoniazid, Rifampicin, and Pyrazinamide) is commenced. Definitive culture at 6 weeks isolates Mycobacterium avium intracellulare. The prescription is altered to include Clarithromycin. Mycobacteria other than the tubercle bacillus sometimes infect humans Atypical Mycobacterial infections in children are most frequently located in the superior anterior cervical or in the submandibular nodes (91%)
Mycobacterium avium complex (MAC) - HIV patients with CD4 < 50
Mycobacterium kansasii
Mycobacterium Marinum * REMEMBER MARINUM = AQUARIUM
Treat with tetracyclines, fluoroquinolones, macrolides, and sulfonamides for 4-6 weeks. |
| Epstein-Barr disease | ReelDx Rotation Room (mononucleosis)Patient will present as → a 14-year-old boy with three days of sore throat, fever, and generalized malaise. On exam, he has a temperature of 102.2 F (39.0 C), BP 96/50, and a diffuse exudate on both tonsils. He is also noted to have palpable splenomegaly, swollen, painful lymph nodes, and mild hepatomegaly. Labs show leukocytosis of 12,000/mm3 with 50% neutrophils, 12% monocytes, and 38% lymphocytes. The rapid pharyngeal streptococcal screen is negative. Epstein Barr mononucleosis is a viral illness characterized by a classic triad of fever + lymphadenopathy + pharyngitis + atypical lymphocytes
DX: Diagnosed with positive heterophile antibody screen (Monospot) - may not appear early in the illness (positive within 4 weeks)
TX: is supportive
|
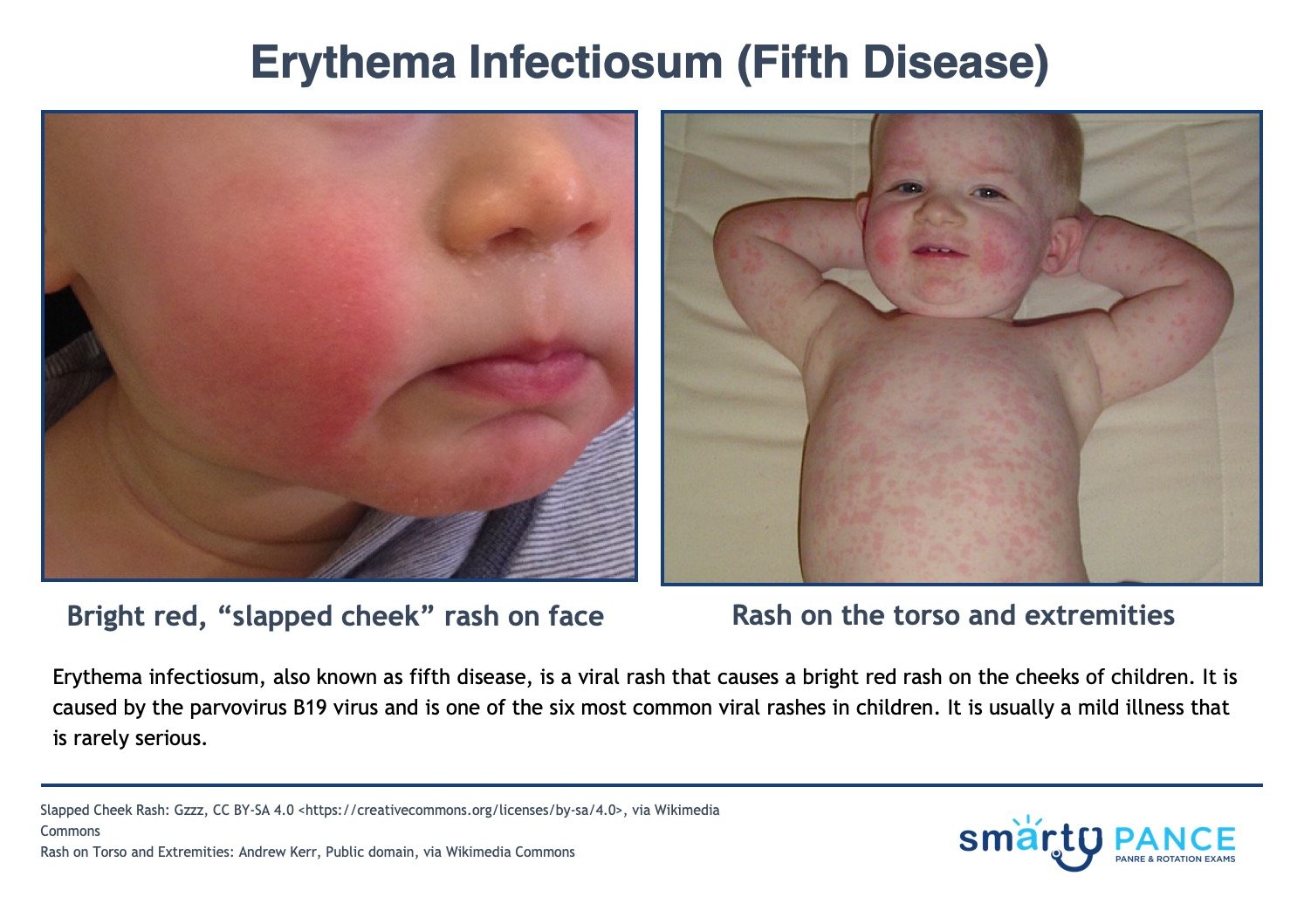
| Erythema infectiosum (fifth disease) | ReelDx Rotation Room (erythema infectiosum)Erythema infectiosum (also known as Fifth's disease) is a common viral exanthem observed in pediatric patients caused by parvovirus B19
DX: is based primarily on clinical observations, history, and physical exam
TX: Treatment is symptomatic
|
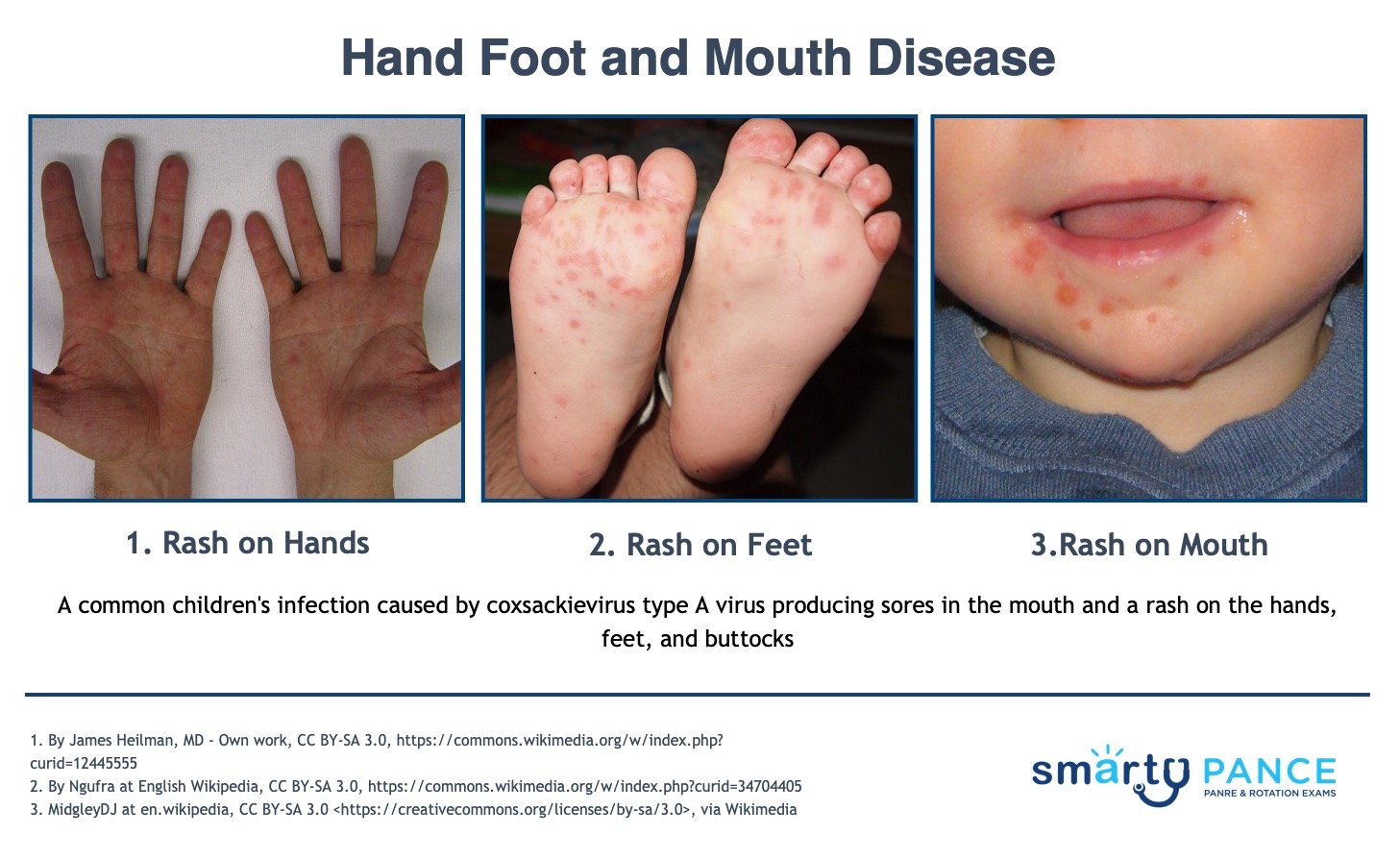
| Hand-foot-and-mouth disease | ReelDx Rotation Room (hand-foot-mouth disease)Patient will present as → a 2-year-old who is brought to the office by his mother. The child has had a low-grade fever, rash, and loss of appetite for the past two days. On physical exam, there are multiple 2-3-mm grey vesicular
lesions on the bilateral palms and soles, and several vesicles and ulcers on the oral mucosa. The PA informs her parents that this disease typically resolves spontaneously and to keep the patient hydrated. A common children's infection caused by coxsackievirus type A virus, producing sores in the mouth and a rash on the hands, feet, mouth, and buttocks
DX: based primarily on clinical observations, history, and physical exam TX: supportive, anti-inflammatories
|
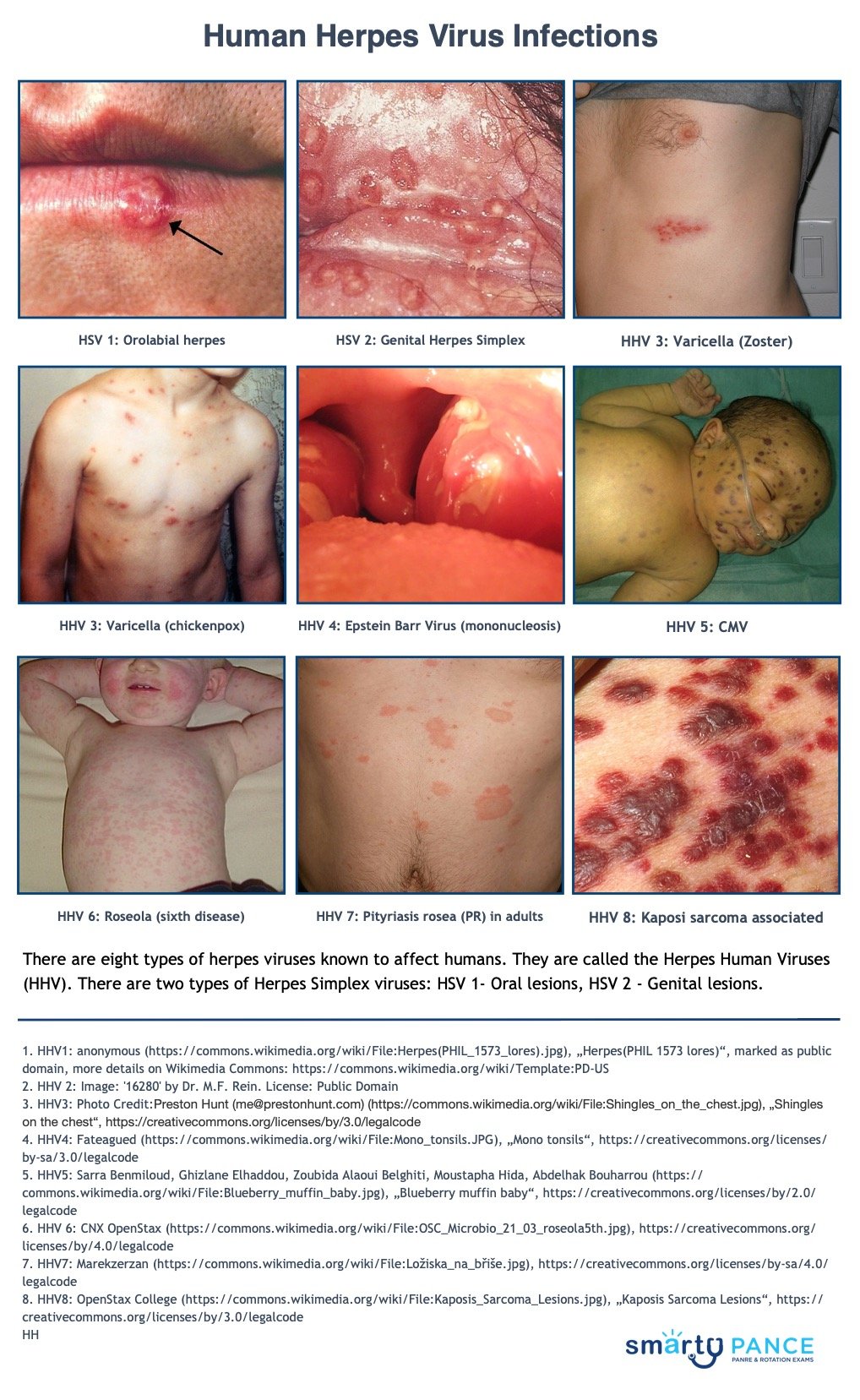
| Herpes simplex | ReelDx Rotation Room (herpes simplex)Patient will present as → a 27-year-old female who complains of exquisite vulvar pain and blisters. She reports that she has experienced several similar episodes for the past 5 years. On examination, you find multiple painful vesicles on her left labia minora. You recall that on a previous visit, she had a positive chlamydia culture that was treated with azithromycin tablets. The Herpes Virus: There are eight types of herpes viruses known to affect humans. They are called Herpes Human Viruses (HHV). There are two types of Herpes Simplex viruses: HSV 1 - Oral lesions, HSV 2 - Genital lesions Herpes Simplex Viruses:
Herpes Human Viruses:
|






| Virus | Name | Conditions |
|---|---|---|
| Herpes simplex virus type 1 | Human herpesvirus 1 | Gingivostomatitis, keratoconjunctivitis, cutaneous herpes, genital herpes, encephalitis, herpes labialis, esophagitis*, pneumonia*, hepatitis* |
| Herpes simplex virus type 2 | Human herpesvirus 2 | Genital herpes, cutaneous herpes, gingivostomatitis, neonatal herpes, aseptic meningitis, disseminated infection*, hepatitis* |
| Varicella-zoster virus | Human herpesvirus 3 | Chickenpox, herpes zoster, disseminated herpes zoster* |
| Epstein-Barr virus | Human herpesvirus 4 | Infectious mononucleosis, hepatitis, encephalitis, nasopharyngeal carcinoma, Hodgkin lymphoma, Burkitt lymphoma, lymphoproliferative syndromes*, oral hairy leukoplakia* |
| Cytomegalovirus | Human herpesvirus 5 | Infectious mononucleosis, hepatitis, congenital cytomegalic inclusion disease, hepatitis*, retinitis*, pneumonia*, colitis* |
| Human herpesvirus 6 | — | Roseola infantum, otitis media with fever; encephalitis |
| Human herpesvirus 7 | — | Roseola infantum and pityriasis rosea, as well as CMV in adults |
| Kaposi sarcoma-associated herpesvirus | Human herpesvirus 8 | Not a known cause of acute illness but has a causative role in Kaposi sarcoma* and AIDS-related non-Hodgkin lymphomas that grow primarily in the pleural, pericardial, or abdominal cavities as lymphomatous effusions Also linked with multicentric Castleman disease |
| *In immunocompromised hosts | ||
View more images of herpes simplex virus infections (HSV1) and (HSV2)
| Influenza | ReelDx Rotation Room (influenza)Patient will present as → a 5-year
-old with sudden onset of fever, chills, malaise, sore throat, headache, and coryza. The child is also complaining of myalgia, especially in her back and legs. On physical exam, the patient appears lethargic, has a temperature of 102.5 F, and palpable cervical lymph nodes. Breath sounds are distant with faint end-expiratory wheezes. Influenza is a viral respiratory infection caused by orthomyxovirus, resulting in fever, coryza, cough, headache, and malaise
DX: usually clinical, rapid antigen tests can be performed in the clinic
Sensitivities of rapid influenza diagnostic tests (RIDTs) are generally approximately 50-70%, but a range of 10-80% has been reported compared to viral culture or RT-PCR. The specificity of RIDTs is approximately 90-95% (range: 85-100%). Thus, false-negative results occur more commonly than false-positive results. TX: Treatment is symptomatic (for most) or with antivirals, ideally< 48 hours. Antiviral treatment reduces the duration of illness by about one day and should be specifically considered for high-risk patients
|
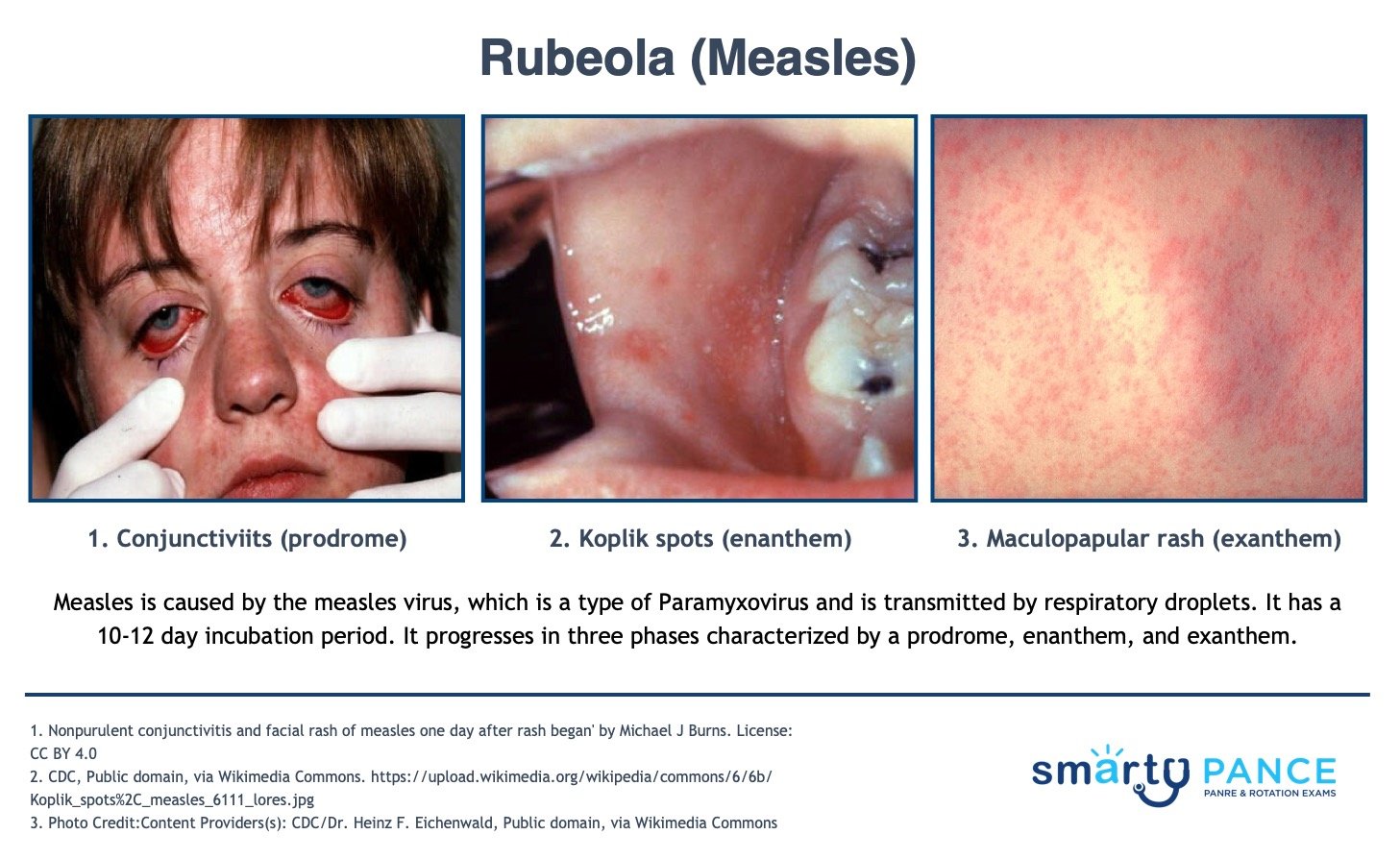
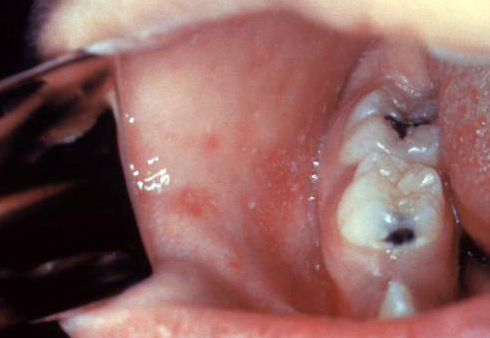
| Measles | Patient will present as → a 6-year-old child who is brought to the emergency room for a complaint of high fevers and a rash. His mother reports that she thought he had “just a cold” approximately one week ago—he had a mild fever, runny nose, conjunctivitis, and cough. Then he developed a rash that started on his face and gradually spread downward. The child has no significant past medical history, however, he was adopted from Russia at age 5, and his medical history prior to adoption is unknown. On examination, the child appears lethargic and has a temperature of 104.3. There is a mild injection of his conjunctiva and a generalized macular rash. White macules are noted on his buccal mucosa. Measles is caused by a paramyxovirus and is transmitted through respiratory droplets; it has an incubation period of 10-12 days. It progresses in three phases characterized by a prodrome, enanthem, and exanthem.
DX: Clinical diagnosis of measles requires a history of fever of at least three days, with at least one of the three C's (cough, coryza, conjunctivitis)
TX: The mainstay of treatment is supportive care and prevention with vaccines - MMR (live attenuated) at 12-15 months, then again at 4-6 years of age
View more images of Rubeola (Measles) |
| Mumps | Patient will present as → a 5-year-old male is brought to the clinic with acute onset of painful swollen parotid glands. His mother reports that he was fine last night, but awoke with the swelling this morning. He has no significant past medical history, but it is documented in his chart that his mother declined the recommended standard immunizations for children because of personal beliefs. On examination, the child appears well and has a temperature of 100.8 F. His right parotid gland is slightly more swollen than the left, but they both are markedly swollen and tender. Mumps is a viral disease that belongs to the Paramyxoviridae family. It presents with parotitis (painful swelling of the parotid gland), orchitis, or aseptic meningitis. It is transmitted through respiratory droplets and has an incubation period of 12-14 days
DX:
TX:
MMR vaccine is given at 12-15 months, then again at 4-6 years of age
|
| Pertussis | Patient will present as → a 24-year-old with an increasing cough for 3 weeks. The cough comes and goes, sometimes lasting for 10 minutes and causing gasping inhalations. The cough was preceded by a mild cough and cold 2 weeks ago. She has completed all immunizations required to attend school and has no known drug allergies Whooping cough (pertussis) is a highly contagious respiratory tract infection marked by a severe hacking cough followed by a high-pitched intake of breath that sounds like a whoop. Gram-negative bacteria Bordetella pertussis – highly contagious
Diagnosed by a nasopharyngeal swab of nasopharyngeal secretions – culture Tx: macrolide (erythromycin/azithromycin); supportive care with steroids / beta2 agonists |
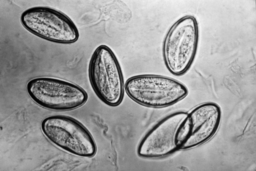
| Pinworms | Patient will present as → a 4-year-old is brought to the office by his mother because the daycare teachers noticed he is unusually restless at school. The mother also noticed that he has not been sleeping well lately and has started wetting the bed at night. The child is alert and cooperative but scratches his buttocks while you are interviewing. Cellophane tape applied to the perianal area reveals football-shaped ova under the microscope. The Scotch tape test</su_spoiler] Pinworm infection, also known as enterobiasis vermicularis, is a human parasitic disease caused by the pinworm (a type of roundworm). The most common symptom is itching in the anal area. This can make sleeping difficult.
DX: "scotch tape test" done in the early morning. You can see the eggs under microscopy TX: albendazole or mebendazole
|
| Roseola | ReelDx Rotation Room (roseola)Patient will present as → a mother who brings her 8-month-old infant into the clinic with a complaint of high fevers for three days. She denies any other symptoms. On examination, the child appears very well and is playful with you despite having a temperature of 103.9 F. A complete physical examination and urinalysis are done, and no source of the fever is found. You send her home with fever control measures and a follow-up appointment for the next day. The next day, the child is afebrile but has a generalized pink maculopapular rash. Roseola, also known as exanthema subitum, roseola infantum, rose rash of infants, sixth disease, baby measles. Caused by HHV 6 and 7
DX: The diagnosis is clinical TX: Treatment is supportive, and in most cases, roseola is a benign and self-limited disease
View more images of Roseola |
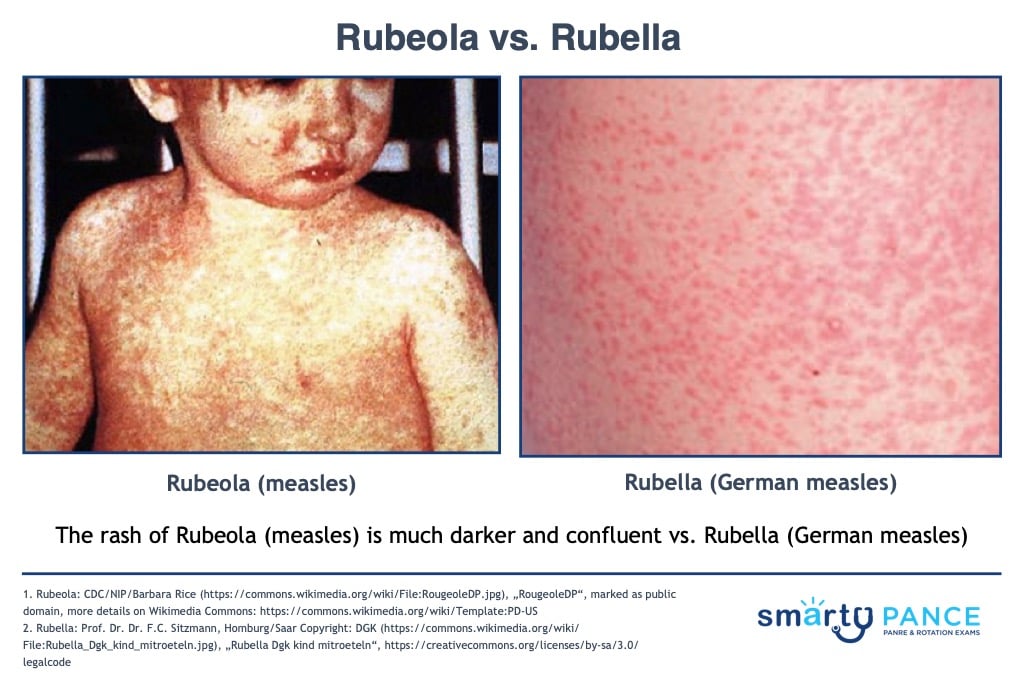
| Rubella | Patient will present as → a mother who brings her 14-month-old daughter for evaluation of a rash. The mother describes the rash as beginning on the face and subsequently spreading to the rest of her body over one day. She also reports that her daughter has a mild fever and redness in her eyes. She has not been vaccinated per her parents’ preferences. The temperature is 100°F (37.8°C). There is mild bilateral nonexudative conjunctivitis, postauricular lymphadenopathy, and petechiae on the soft palate and uvula. Pink maculopapules are found in the face, neck, trunk, and extremities. The rash disappears in three days.
DX: Laboratory diagnosis of rubella is warranted when congenital rubella syndrome is suspected or when the diagnosis is sought for a condition compatible with the known complications of postnatal rubella, such as arthritis
Tx: The mainstay of treatment is supportive care and prevention with vaccines - MMR (live attenuated) at 12-15 months, then again at 4-6 years of age
Distinguish from measles by → confluent maculopapular rash, coryza (stuffy nose), and Koplik spots (in measles) |
| Varicella infection | ReelDx Rotation Room (Chicken Pox)Varicella (chickenpox): primary infections - clusters of vesicles on an erythematous base Patient with varicella (chickenpox) will present as → a 3-year-old with fatigue, irritability, and a low-grade fever that he has had for 3 days. According to the patient’s mom, the child attends a daycare where a virus is “going around.” On physical examination, the child does not look ill. His temperature is 98.6 F (38 C). His skin examination shows scattered, small vesicles on an erythematous base. The rash was seen first on the face and seems to be spreading to the trunk.
ReelDx Rotation Room (Shingles)Herpes zoster (shingles): varicella reactivation causing a maculopapular rash along one dermatome Patient with herpes zoster (shingles) will present as → a 67-year-old male who presents to your clinic with a two-day history of a painful rash on his left flank radiating to his back. This was preceded by burning pain in the same region several days prior. The patient does not recall any history of childhood exanthems and is not up to date on his immunizations. Vital signs are stable. Physical exam reveals a maculopapular rash in a dermatomal distribution on the left flank and extending into the back.
Vaccination:
|









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}