


5 y/o with fever and emesis
Patient will present as → a 5-year-old with sudden onset of fever, chills, malaise, sore throat, headache, and coryza. The child is also complaining of myalgia, especially in her back and legs. On physical exam, the patient appears lethargic, has a temperature of 102.5 F, and palpable cervical lymph nodes. Breath sounds are distant with faint end-expiratory wheezes. CXR demonstrates bilateral diffuse infiltrates.
Influenza is a viral respiratory infection caused by orthomyxovirus resulting in fever, coryza, cough, headache, and malaise - three strains exist: A, B, and C
- Patients will present with fever, headache, myalgia, and malaise
- Complications from influenza are most common in the very young, very old, and those with preexisting comorbidities
- The CDC recommends routine annual influenza vaccination is recommended for all persons aged ≥6 months who do not have contraindications
- Antivirals are most effective if administered within the first 48 hours and reduce the duration of illness by about 1 day
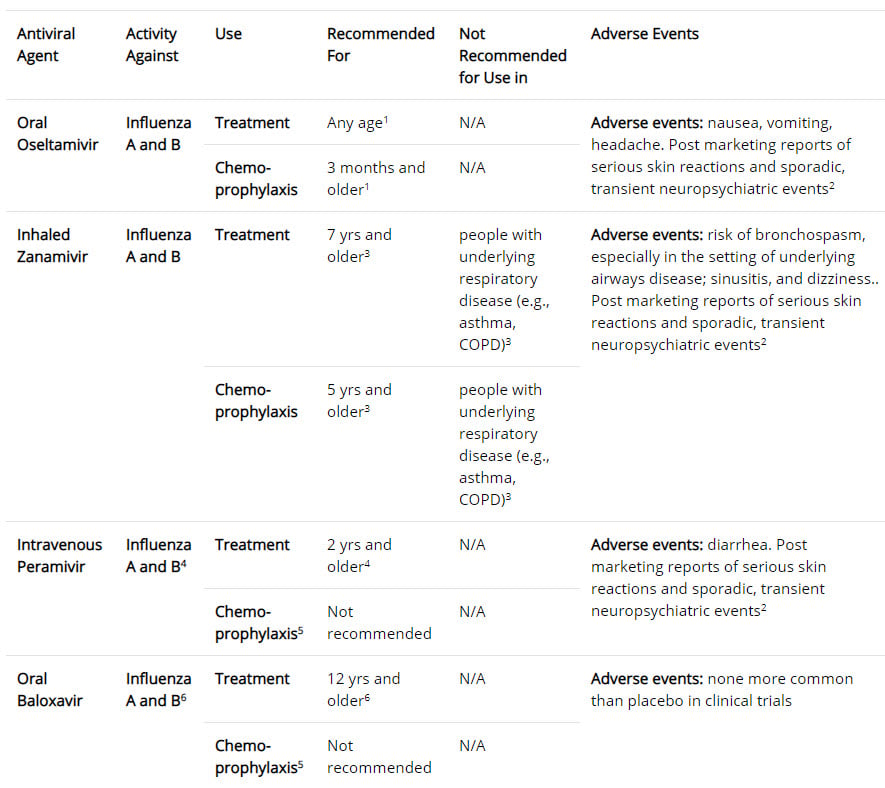
- Four antiviral medications approved by the U.S. FDA are recommended for use during the 2019-2020 influenza season
- Inhaled Zanamivir (Relenza), oral Oseltamivir (Tamiflu), and intravenous peramivir (Rapivab) are all neuraminidase inhibitors and treat influenza A and B
- The fourth drug which is oral baloxavir (Xofluza), is active against both influenza A and B viruses and is a cap-dependent endonuclease inhibitor that interferes with viral RNA transcription and blocks virus replication
- Amantadine and Rimantadine are in a class of medications known as adamantanes, which target the M2 ion channel protein of influenza A viruses
Diagnosis is based primarily on patient history. A rapid antigen test can be performed in the clinic - the virus can be isolated from the throat or nasal mucosa
- Rapid serology tests are often available and are most accurate during the first few days of illness
- Gold standard = RT-PCR or viral culture takes 3-7 days to return
- CXR in primary influenza pneumonia will show bilateral diffuse infiltrates
{kind=link}

Chest radiograph from a patient with viral pneumonia showing widespread bilateral interstitial infiltrates
Best to treat with medications if symptoms are less than 48 hours in duration (although there are exceptions to this rule). Six licensed prescription influenza antiviral drugs are approved in the United States.
Four antiviral medications approved by the U.S. FDA are recommended for use during the 2019-2020 influenza season.
- Three drugs are neuraminidase inhibitors that block the viral neuraminidase enzyme and have activity against both influenza A and B viruses:
- Oral oseltamivir (Tamiflu) – dosed at 75 mg PO two times per day for 5 days. Prevention – 75 mg once daily x 10 days within 48 hours of exposure
- Inhaled zanamivir (Relenza) – 2 puffs two times per day for 5 days. Prevention – 2 puffs once daily x 10 days within 48 hours of exposure
- Intravenous peramivir (Rapivab) – 600 mg IV once daily x 5 days (for hospitalized patients who cannot take PO oseltamivir)
- The fourth drug which is active against both influenza A and B viruses is a cap-dependent endonuclease inhibitor that interferes with viral RNA transcription and blocks virus replication
- Oral baloxavir (Xofluza) – 40 mg single dose 40-80 kg. 80 mg for > 80 kg
*** Zanamivir and Oseltamivir both treat influenza A and B (think Dr. “OZ” treats the flu)
Amantadine and Rimantadine are in a class of medications known as adamantanes, which target the M2 ion channel protein of influenza A viruses
- Amantadine and rimantadine are not recommended for antiviral treatment or chemoprophylaxis of currently circulating influenza A viruses
The use of salicylates should be avoided, particularly in children below 18 years of age, because of association with Reye's syndrome. Remember Bismuth contains salicylates, should be avoided and could be a cause of Reye's syndrome.
Responsible use of antivirals:
- Antiviral treatment depends on current resistance patterns each year; check www.cdc.gov/flu or the local health department for current patterns. Antivirals are most effective if administered within 1st 48 hours in those with laboratory-confirmed (or highly suspected based on clinical findings) influenza illness.
- Antivirals within 48 hours of symptom onset are recommended if at risk of complications (ie. Diabetes, CHD, COPD, Asthma, etc.)
- Antivirals recommended if hospitalized
- Antivirals may be considered for persons not at increased risk of complications from influenza whose onset of symptoms is within the past 48 hours and who wish to shorten the duration of illness and further reduce their relatively low risk of complications.
- Symptomatic treatment is preferred for those patients without risk factors and without signs of lower respiratory tract infection
CDC GUidelines for influenza outbreak management in long-term care facilities and post-acute care facilities
When at least 2 patients are ill within 72 hours of each other and at least one resident has laboratory-confirmed influenza, the facility should promptly initiate antiviral chemoprophylaxis with oral oseltamivir to all non-ill residents living on the same unit as the resident with laboratory-confirmed influenza (outbreak affected units), regardless of whether they received influenza vaccination during the current season.
- Consideration may be given for extending antiviral chemoprophylaxis to residents on other unaffected units or wards in the long-term care facility based upon other factors (e.g. unavoidable mixing of residents or staff from affected units and unaffected units).
 Osmosis Osmosis |
|
 |
Influenza, commonly called the flu, is an infectious disease caused by an RNA virus of the Orthomyxovirus family. This is an enveloped virus with single-stranded negative sense linear genome. The genome is also segmented into 8 segments and has helical protein capsid. Virulence mechanisms include hemagglutinin, which is an antigenic glycoprotein found on the surface of influenza viruses that aids in viral entry of a cell and neuraminidase, an enzyme that plays an important role in the release of virion progeny from infected cells. This virus has the capacity to undergo reassortment of the genome to cause major changes in the strain of influenza. This major change is commonly referred to as genetic shift and can be highly dangerous because the human immune system has difficulty recognizing the new strain of the virus. In contrast, genetic drift refers to minor antigenic mutations that occur and are associated with gradual loss of immunity. Common symptoms of influenza virus include chills, fever, sore throat, muscle pains, headache, and fatigue. Complications include Reye’s syndrome, a potentially fatal disease commonly associated with salicylate use in children with influenza, and the virus can also be a trigger for Guillan-Barre.
Play Video + QuizZanamivir (Relenza) and Oseltamivir (Tamiflu)

Zanamivir (Relenza) and Oseltamivir (Tamiflu) are antiviral medications used to treat and provide prophylaxis against influenza A and B. These drugs work by binding to neuraminidase, preventing the virus from escaping its host cell and infecting others.
Reye’s syndrome
Reye’s syndrome is a disorder associated with salicylate use in children with viral illnesses, such as the chickenpox and influenza. For this reason, aspirin and other NSAIDs should be avoided in this population. Instead, acetaminophen can be used. This syndrome is known to affect various organs throughout the body including fatty changes in the liver. As the child’s liver begins to fail, lab results may show increased liver enzymes, such as AST, ALT, and increased ammonia levels. Reye’s syndrome is characterized by acute encephalopathy. Children should be monitored closely for signs of increasing ICP, such as a change in level of consciousness, headache, vomiting, abnormal/asymmetrical pupils, posturing, and/or seizures. Early detection and treatment of Reye’s syndrome is essential, as death may result within hours if left untreated.
Play Video + QuizQuestion 1 |
Amantadine (Gocovri) Hint: Amantadine and rimantadine are NOT recommended for use because of high levels of antiviral resistance to these drugs among circulating influenza A viruses. | |
Oseltamivir (Tamiflu) | |
Rimantadine (Flumadine) Hint: Amantadine and rimantadine are NOT recommended for use because of high levels of antiviral resistance to these drugs among circulating influenza A viruses. | |
Baloxavir (Xofluza) Hint: Baloxavir is not approved for chemoprophylaxis of influenza and is not recommended for chemoprophylaxis of influenza in long-term care facility residents. |
Question 2 |
azithromycin (Zithromax) Hint: See D for explanation. | |
acyclovir (Zovirax) Hint: See D for explanation. | |
tetracycline (Sumycin) Hint: See D for explanation. | |
zanamivir (Relenza) |
Question 3 |
Amantadine (Symmetrel) Hint: Amantadine is only used to treat influenza A. | |
Oseltamivir (Tamiflu) | |
Acyclovir (Zovirax) Hint: Acyclovir is used to treat viral infections due to certain herpes viruses. | |
Nevirapine (Viramune) Hint: Nevirapine is used to treat infection due to HIV. |
|
List |
References: Merck Manual · UpToDate