Patient will present as → a 67-year-old female with a history of hypertension, hyperlipidemia, and coronary artery disease presents to the clinic with poorly controlled blood pressure despite being on three antihypertensive medications. She reports frequent headaches and dizziness and notes that her blood pressure has been fluctuating for the past few months. On physical examination, her blood pressure is 180/95 mmHg, and there is an audible abdominal bruit over the epigastric area. Laboratory results show a mild elevation in serum creatinine. A renal duplex ultrasound reveals significant renal artery stenosis. Further evaluation with CT angiography confirms a 70% narrowing of the left renal artery. The patient is diagnosed with renal vascular disease, specifically renal artery stenosis, likely secondary to atherosclerosis. Management includes lifestyle modifications such as smoking cessation, a heart-healthy diet, and regular exercise. Medications, including statins, are started to reduce cholesterol, and antihypertensive therapy is optimized. Given the severity of stenosis and her uncontrolled blood pressure, the patient is referred for percutaneous transluminal renal angioplasty (PTRA) with or without stent placement. Long-term follow-up includes monitoring of renal function, blood pressure, and the success of revascularization.
Renal artery bruit (with bowel sounds)
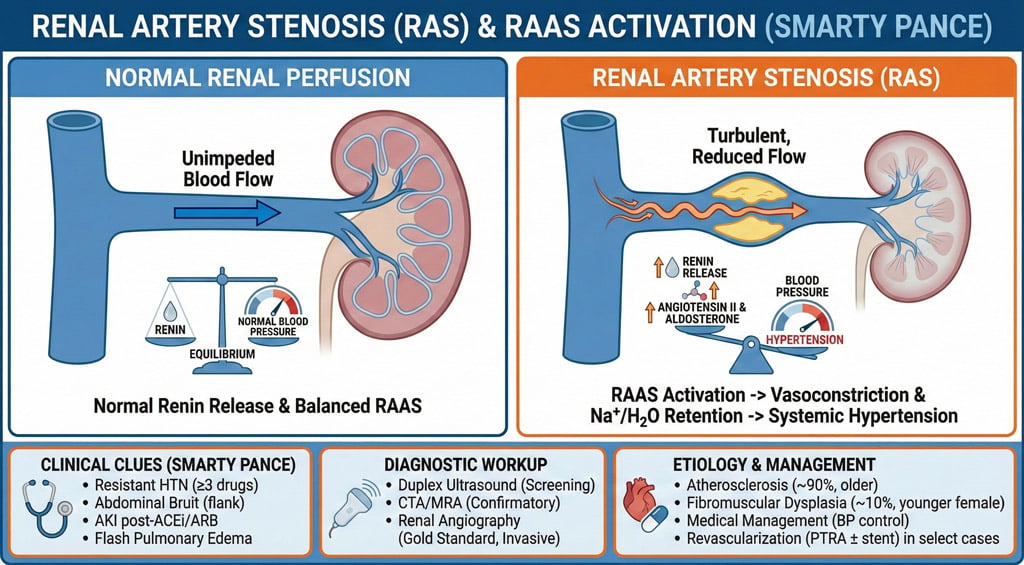
Renal artery stenosis is the narrowing of one or both renal arteries, most often caused by atherosclerosis or fibromuscular dysplasia
- Narrowing of the renal artery can impede blood flow to the target kidney
- The reduced blood flow is interpreted by the kidneys as a sign of low blood pressure, triggering the renin-angiotensin-aldosterone system (RAAS). This leads to increased sodium and water retention and vasoconstriction, ultimately resulting in renovascular hypertension (a secondary type of high blood pressure)
May hear a renal artery bruit on auscultation
- Patients may present with HTN before age 30, HTN with CAD or PVD history, or hypertension resistant to three or more drugs
- If a patient is placed on an ACE inhibitor and suddenly develops acute renal failure or a sharp rise in BUN/CR, you should think of renal artery stenosis
Renal Doppler ultrasound is often the initial imaging in those < 60 years of age with suspected RAS
- Renal arteriography is the GOLD STANDARD for diagnosis

Renal arteriography demonstrating renal artery stenosis
Stenting of renal arteries
- Treatment is with percutaneous transluminal angioplasty (PTA) plus stent placement or with surgical bypass of the stenotic segment
- Usually, an extensively infarcted kidney must be removed if revascularization is not expected to result in functional recovery
- In patients with renal artery stenosis, especially those with stable renal function, the most appropriate initial management is medical management with antihypertensive medications
- ACE inhibitors and ARBs can be used in unilateral and, if glomerular filtration rate (GFR) is monitored closely, in bilateral renal artery stenosis
- Additional antihypertensive medications are frequently required
 Osmosis Osmosis |
|
 |
Question 1 |
Acute glomerulonephritis Hint: Usually presents with hematuria, proteinuria, and sometimes hypertension, but not typically with sudden severe hypertension. | |
Renal artery stenosis | |
Chronic kidney disease Hint: Develops gradually and is not typically associated with sudden severe hypertension. | |
Renal cell carcinoma Hint: Can cause flank pain and hematuria, but sudden severe hypertension is less common. | |
Pyelonephritis Hint: Presents with fever, flank pain, and urinary symptoms, not typically with severe hypertension. |
Question 2 |
Renal ultrasound with Doppler Hint: Useful but less sensitive than CT angiography for detecting renal artery stenosis. | |
CT angiography of the renal arteries
| |
Magnetic resonance angiography (MRA) of the renal arteries Hint: An alternative to CT angiography but may be less available or contraindicated in some patients. | |
Renal biopsy Hint: Not indicated in the initial evaluation of renal artery stenosis. | |
24-hour urine collection for metanephrines Hint: Used to diagnose pheochromocytoma, not renal artery stenosis. |
Question 3 |
Medical management with antihypertensive medications | |
Immediate surgical revascularization Hint: Considered in cases with refractory hypertension or deteriorating renal function. | |
Percutaneous transluminal renal angioplasty with stenting Hint: An option for certain patients, particularly those with fibromuscular dysplasia or those who fail medical therapy. | |
Chronic dialysis Hint: Indicated in end-stage renal disease, not as initial management for renal artery stenosis. | |
Nephrectomy Hint: Not a treatment for renal artery stenosis. |
Question 4 |
Hydrochlorothiazide-Triamterene | |
Prazosin Hint: An alpha-blocker like prazosin is generally safe in renal artery stenosis and does not directly worsen renal function. | |
Nifedipine Hint: This calcium channel blocker is often used to manage hypertension and does not have a direct deleterious effect on renal artery stenosis. | |
Verapamil Hint: Another calcium channel blocker, verapamil is typically safe in patients with renal artery stenosis. | |
Furosemide Hint: While loop diuretics like furosemide can be used cautiously in renal artery stenosis, they are not contraindicated as thiazide diuretics are. |
|
List |
References: Merck Manual · UpToDate