Welcome to episode 92 of the Audio PANCE and PANRE physician assistant/associate board review podcast.
Today is part two of this extraordinary five-part series with Joe Gilboy PA-C, all about cardiac murmurs. In this week's episode of the Audio PANCE and PANRE podcast, we continue our discussion of cardiac murmurs with a focus on the mitral valve.
We'll talk about the different types of murmurs (stenosis and regurgitation) that can occur with this valve and how to differentiate them from other types of murmurs. If you haven't already, make sure to listen to our previous podcast episode where we covered the aortic valve murmurs.
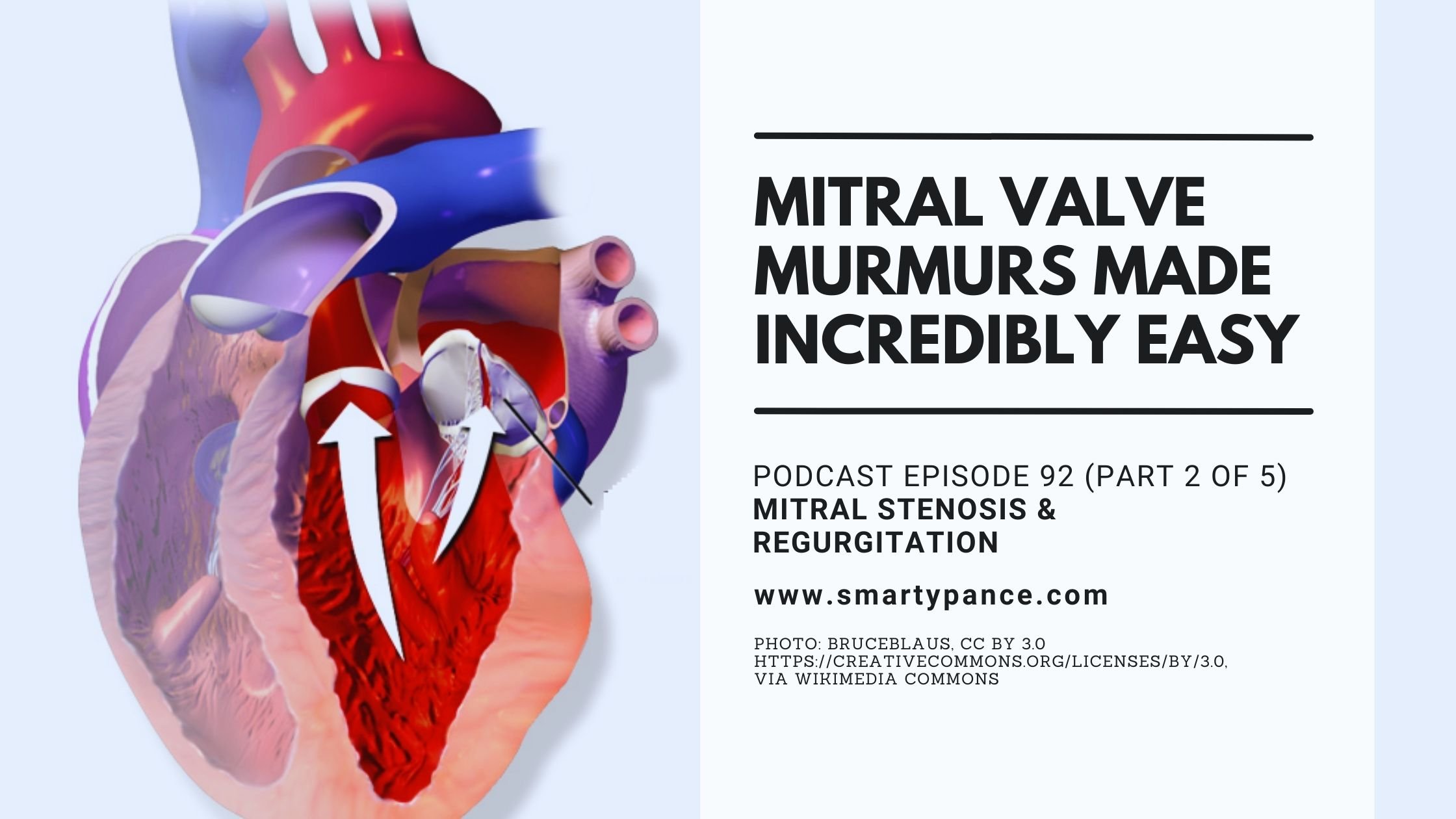
The Mitral Valve
The mitral valve is located between the left atrium and the left ventricle in the heart. It consists of two leaflets (or cusps) and is responsible for preventing blood from flowing back into the atrium when the ventricle contracts.
The mitral valve can have two types of murmurs: stenosis and regurgitation.
- Mitral stenosis is a narrowing (or constriction) of the valve opening, which reduces the amount of blood that can flow through the valve. This type of murmur is of low pitch, rumbling in character, and best heard at the apex with the patient in the left lateral position.
- Mitral regurgitation is a leakage (or backflow) of blood from the ventricle into the atrium, caused by weakened or damaged valve leaflets. This type of murmur is a holosystolic (pansystolic) murmur, heard best at the apex with the diaphragm of the stethoscope when the patient is in the left lateral decubitus position.
In addition to auscultation, you can also look for certain signs and symptoms that may indicate mitral stenosis or regurgitation. For example, if a patient presents with chest pain (angina pectoris), this could be from decreased oxygen supply due to poor cardiac output in cases of significant stenosis. On the other hand, if a patient presents with an irregular heart rate (arrhythmia), this could be from increased electrical conduction velocity in cases of significant regurgitation.
Also, keep in mind that mitral valve disease can also occur secondary to rheumatic fever or endocarditis, so you may need to consider these diagnoses if a patient has any of the aforementioned signs and symptoms.
Below is a transcription of this podcast episode edited for clarity.
- You can download and listen to past FREE episodes here, on iTunes, Spotify, Google Podcasts, Stitcher, Amazon Music, and most podcasting apps.
- You can listen to the latest episode and access even more resources below.
Welcome, everybody. This is Joe Gilboy, and I work with Stephen Pasquini at Smarty PANCE.
Today we're back to the heart murmur podcast, and we just finished the aortic valve. The next one up is the mitral valve.
Let's just look at this my way. In school, you memorize a bunch of facts, then someone asks a question about mitral stenosis or mitral regurgitation, and you are completely lost. It's time to change that. Now, we are going to do it my way. Are you ready? Here we go.
Let's look at the mitral valve on a normal day. What's the mitral valve doing?
- There is my left atria. It's contracting during diastole, my mitral valve opens up, and the blood flow goes to the left ventricle.
- Then during systole, the mitral valve will close, the left ventricle will squeeze, and the aortic valve opens.
Mitral Valve Stenosis

Let's start with the first heart murmur, mitral stenosis. Think about it. Slow down and give this some thought.
I've got the stenotic mitral valve. See it? It can barely open. It's like, man; you've got to push hard to open this door. So, you are the left atrium, and you're pushing down on this stenotic mitral valve. It's like, man; this is hard to open up! I have to push harder. Yes, you do!
Wait for a second; then I'm going to put more blood flow back against my left atrium? Completely correct. So, my left atrium might hypertrophy? Yes, that's correct!
So, you're telling me I might get left atrial hypertrophy with mitral stenosis? Exactly!
Now, think about it. There you are in the left atrium pushing against the mitral valve during stenosis that's supposed to open during diastole. You're just taking longer to open up. You see, in school, what you memorize is an opening snap. Remember that ridiculous graph where you saw it had S1, S2 on all those bar graphs? You thought you were reading a musical sheet. Do you remember that thing? Or you're like oh, S1 S2 ..........!? You were looking at it thinking, " I have no fricking idea what I'm looking at." Let's erase that.
Think about this for a second; if the left atrium is pushing on a stenotic valve, it's going to have trouble during diastole. Because during systole, it has to be closed. It's going to close without a problem. The problem is opening it up. You can see the left atrium hypertrophy. Then blood flow may back up into the lungs and causes pulmonary hypertension.
Oh, wait for a second, I get pulmonary hypertension? Yes, you do!
Then maybe I have some fluid backed up in the lungs, and I might have a little shortness of breath and CHF. Exactly! Yes, that's exactly how they're going to present.
So, I have this diastolic murmur. It's a diastolic ejection murmur to open that valve up. So, it's not going to be an accentuated S1. But that's not what they're going to say on your boards, are they? No, that's just a buzzword.
What they're going to say is, "I have this diastolic rumbling murmur." Rumbling means I'm trying to open up, and I'm going to radiate down towards the apex. That just makes logical sense.
So, I have this diastolic murmur radiating to the apex. Let's take a closer look at the mitral valve. Remember, your heart doesn't sit flat. It sits tilted towards the back. So, I need this mitral valve to get towards the front. Okay, well, then tilt yourself to the left and lay down. Oh! That's that left lateral to decubitus position they keep talking about. I'm going to bring it closer to the front.
Oh, that makes sense. I totally see that. So, I have a diastolic murmur that radiates to the apex. I can hear it better if I lay down on the left lateral decubitus position because that will bring the valve closer to the chest. Let's make it sound louder now.
Okay, one more time back to how we were in the beginning with the aortic valve. Okay, what's your party maneuver? Oh, I want to party, and I want to bring all the blood flow back home. How do you party? Oh, I squat. Squatting is a party. So, what are you going to do if I squat? How's mitral stenosis sound? Louder! I get more blood flow pushing against the stenotic valve.
If I perform low-volume maneuvers, which are standing and Valsalva, I get less blood to the heart. Hi, standing and Valsalva, what's going to happen to mitral valve stenosis? Yes, it's going to go away!
Inspiration => right (louder), and expiration => left (louder). Repeat: inspiration right and expiration left. Hi, I have mitral stenosis! Oh, he's on the left. What's going to make him sound louder? Expiration? Yes, exactly!
Now, does everyone see this? So, you see, they're not going to give you that "opening snap" buzzword. All the buzzwords on the PANCE are gone, guys, so just throw them away. What they're going to give you is some person with a heart murmur, who maybe has a little CHF, has a diastolic murmur, and that's it. That's all they're going to give you now. What you have to think is diastolic: left side, going back to the lungs = stenosis. That makes perfect sense. And that's mitral stenosis. So, the "open snap," those buzzwords are gone.
Let's review one more time:
- How do I make mitral stenosis sound louder? Squatting.
- Inspiration (right) and expiration (left) => If the murmur is on the left (the mitral valve is on the left) => expiration makes it sound louder.
- Standing and Valsalva are low-volume maneuvers, and the murmur of mitral stenosis goes away.
- How do I hear mitral stenosis better? I need to put the murmur towards the chest. Well, the heart is lying towards the back, so I need to lay it towards the front so I can hear the murmur better. The lateral decubitus position repositions the mitral valve towards the front. That makes so much sense.
There you go, that's mitral stenosis.
Mitral valve stenosis can be heard best with the patient in the left lateral decubitus position
- How do you hear mitral stenosis better? You need to put the murmur towards the chest. The heart is lying towards the back, so if you lay it towards the front, you can hear the murmur better. The lateral decubitus position repositions the mitral valve towards the front.
Standing and Valsalva (low volume maneuvers that decrease venous return/preload): (↓) MS murmur
- The murmur of MS diminishes in intensity due to reduced venous return to the heart with standing and Valsalva.
Squatting and leg raise (high volume maneuvers that increase venous return/preload): (↑) MS murmur
- The murmur of MS becomes louder with squatting (or passive leg raising) because more blood is coming back to the heart. Although as mitral regurgitation becomes more severe, the murmur may increase in intensity with squatting due to an increase in afterload.
Sustained hand grip (increase afterload): Negligible effect in MS
- Since increasing afterload will prevent blood from flowing in a normal forward path, it will increase any murmurs that are due to backward-flowing blood. It has a negligible effect on mitral stenosis.
Respiration: (↑) MS murmur with Expiration
- Left-sided heart murmurs increase with expiration. Right-sided murmurs (e.g., tricuspid regurgitation) increase with inspiration due to increased venous return to the right heart.
Mitral valve regurgitation

Then there's mitral valve regurgitation. I want you to view mitral regurgitation as "come and go as you please."
This is a valve that won't close. Repeat, "come and go as you please." Let's review the mitral valve again. "Hi, I'm diastole, I'm the left atria, and I'm coming through a valve that doesn't care. Do you have any problems? No, I'm supposed to be open. So, I'm coming through during diastole not a problem."
Now, let's compare that to systole: "Hi, I'm systole and that mitral valve is supposed to be closed." But is it going to be closed? Nooo. In systole, blood is coming and going as it pleases. So, wait for a second, then I'm going to be a systolic murmur. 100% correct. And are you having any resistance? Zero.
That's why we call it a holosystolic murmur. Understand? And now I'm going from the apex at the bottom of the heart, and I'm radiating to the axilla. So, you're going back up to the left atrium? Exactly.
So how is your blood flow out to the rest of the world? Not that good. Not good at all. So how are you feeling? I'm feeling a bit lightheaded (syncope) and short of breath.
Now let's go one step further. Remember that LAD, the Windowmaker? Okay, if you look at the left anterior descending artery, it bifurcates into the left anterior descending and septal branches. Both these guys feed the chordae tendineae. It's that octopus-looking muscle that pulls the mitral valve down. So now think about this for a second. Just give us some thought. Ready?
You just had a LAD MI. You're in the hospital. The cardiologist has just put down a stent. You're on the heparin drip. You are getting ready to go home, maybe on Xarelto or Eliquis.
So, there you are, on a blood thinner. Can I ask you a question? Just give it a thought. You know, your chordae tendineae? You know, during the MI, remember that? Yes, you're lacking blood flow to the left ventricle, aren't you? Yes. How is your blood flow to your chordae tendineae? Yes, it was diminished.
Let's review. The patient is in the hospital and on an IV beta-blocker (you want to rest the heart). Well, they're going home and back to activities like walking through Costco or Walgreens, or CVS. He's no longer on a beta blocker, folks. His heart rates back up.
Is this chordae tendineae ready for a normal heart rate? Yes, or no? No, not at all. He's on the injured reserve list as well. And guess what? His chordae tendineae is not going to hold very well. He says, "Oh my god, I'm so weak. I can't hold the mitral valve down". Which means it is going to open back up.
That's the test question you will see - it is the post-MI patient who comes in two to four weeks later. The patient who's got a new-onset murmur. What does he have? He's got mitral regurgitation because his chordae tendineae got hypoxic during the MI, and now he's got the murmur. So that's a question that you see on Rosh Review, Hippo, Smarty PANCE, UWorld, and Kaplan. You'll see this question rear its head, but the root of what they're really after is something else.
They want you to understand that the chordae tendineae itself was actually lacking blood flow during the LAD or ischemic event. So, it's weakened. As soon as the patient goes to stress it out, it's not going to work very well. It's going to give way, and the chordae tendineae will rupture. What you have is mitral valve regurgitation. Does everybody see this?
Standing and Valsalva (low volume maneuvers that decrease venous return/preload): (↓) MR murmur
- The murmur of MR diminishes in intensity due to reduced venous return to the heart with standing and Valsalva.
Squatting and leg raise (high volume maneuvers that increase venous return/preload): (↑) MR murmur
- The murmur of MR becomes louder with squatting (or passive leg raising) because more blood is coming back to the heart. Although as mitral regurgitation becomes more severe, the murmur may increase in intensity with squatting due to an increase in afterload.
Sustained hand grip (increase afterload): (↑) MR murmur
- Hand grip (sustained for 20 to 30 seconds) is most useful in differentiating the ejection systolic murmur of aortic stenosis from the murmur of mitral regurgitation: The intensity of the murmur of aortic stenosis tends to decrease, while the murmur of mitral regurgitation increases.
- With hand grip, imagine someone sitting on the aortic valve. There is more pressure resisting blood flow from the left ventricle through the aortic valve – thus more blood flow and pressure regurgitates through the mitral valve during systole.
- Since increasing afterload will prevent blood from flowing in a normal forward path, it will increase any murmurs that are due to backward-flowing blood.
Respiration: (↑) MR murmur with Expiration
- Left-sided heart murmurs increase with expiration. Right-sided murmurs (eg, tricuspid regurgitation) increase with inspiration due to increased venous return to the right heart.
So, as a recap, let's look at this again.
- What's the mitral valve supposed to do? Well, I suppose you'd say, "to open up during diastole and close during systole."
- I see that I've got mitral stenosis. What's your problem? Well, my problem is during diastole. It's trying to open the thing up. Because during systole, don't worry, it will close. It's stenotic. It wants to stay closed. So, my problem is during diastole. They will not use the words "diastolic opening and snap." But they may use the word "rumbling murmur."
- Where's the blood flow backing up to? The left atria.
- What's the left atria going to do? Hypertrophy. What are you going to get? Left atrial hypertrophy.
- Where's the blood flow going to back up to? It's going back up to the lungs. What do you have? Pulmonary hypertension.
- What do you get? CHF.
This is the test question you're going to get. An immigrant comes in with a diastolic murmur and shortness of breath. We don't have the best testing for strep. Remember rheumatic fever? They are in their 30s and 40, and they've had rheumatic fever in the past, with mitral stenosis, and now the fluid is backing up to the lungs. That's why they have shortness of breath.
- Now, how do you make that murmur sound louder? Inspiration (right) and expiration (left) => If the murmur is on the left (the mitral valve is on the left) => So expiration makes it sound louder.
- Squatting, it's a party, and the murmur gets louder! Standing and Valsalva, it goes away!
- Is your problem during diastole with mitral regurgitation? It's like, come and go as you please. You know, let's open and come on in. What's your problem during systole because you should close... what he's doing? You see, I don't care. I can come and go as you please. So, my problem is going to be during systole.
- So mitral regurgitation is going to be a holosystolic murmur.
- And then, make it sound louder. Squatting is a party. Standing and Valsalva are low volume maneuvers. It goes away. Exactly!
And that's the point I'm trying to make about the mitral valve. Does everybody see that now?
When you get the test questions, stop and think. You're going to laugh because one of the things I tell all my students to do all the time is to try to make sense of it. See, what you guys do is memorize these things, and you run into your, what I call your data closet. I call it a closet full of data.
You get into this data closet, and what happens is you get lost in the closet. You say to yourself, "Okay, diastolic murmur, axilla blah, blah, blah, what did I memorize? Let me write down my little mnemonic. Yes, yes. Oh, man, I can't Oh, man." Next, you're just panicking. And you just choose A, B, C, or D.
You say to yourself, "oh my god, I think I got the question wrong." Exactly.
So next time, just try making sense of it.
So, we did the aortic valve, and we did the mitral valve. So, we did everything on the left. Next week, we are going to the right folks. We're going to go to the pulmonic valve and the tricuspid valve.
So, one more time, guys. Inspiration right, expiration left. Inspiration right, expiration left. To make the right side of your heart murmur sound better, what are you going to do? Inspiration, so pulmonic and tricuspid sound louder with inspiration.
Expiration left. Who sounds better on the left? Aortic and mitral!
It's been an honor and a pleasure talking with you today. I hope this makes more sense. Next week we'll do the pulmonic valve. Till then, be good to yourself and take care.
Joe Gilboy PA-C
Resources and links from the show
- Download your Free interactive PANCE, PANRE, and EOR Blueprint Templates
- Follow Smarty PANCE and The Daily PANCE Blueprint on Instagram and Facebook
- Check out my list of recommended PANCE and PANRE review books
- Sign up for the FREE Daily PANCE and PANRE email series
- Join the Smarty PANCE NCCPA Content Blueprint Website
- Get your free 8-week PANRE Blueprint study schedule and the 8-week PANCE study schedule
- Get your free Trello PANCE study planner
- Get 20% off any Picmonic membership by using this link, or if you are a Smarty PANCE member, get Picmonic for Smarty PANCE.
This podcast is available on every device.
You can download and listen to past FREE episodes here, on iTunes, Spotify, Google Podcasts, Stitcher, Amazon Music, and all podcasting apps.
Download the Interactive Content Blueprint Checklist
Follow this link to download your FREE copy of the PANCE/PANRE/EOR Content Blueprint Checklists.
Print it up and start crossing out the topics you understand, marking the ones you don't, and making notes of key terms you should remember. The PDF version is interactive and linked directly to the individual lessons on Smarty PANCE.
Image attribution: Blausen.com staff (2014). "Medical gallery of Blausen Medical 2014". WikiJournal of Medicine 1 (2). DOI:10.15347/wjm/2014.010. ISSN 2002-4436. Crop by Stephen Pasquini PA-C, CC BY 3.0


