


60 y/o with abdominal pain, vomiting, and altered mental status
{kind=link}
Audio: Severe mitral stenosis and regurgitation (rheumatic origin)

To watch this and all of Joe-Gilboy PA-C's high-yield video lessons, you must be a member. Members can log in here or join now.
Infective endocarditis is an infection of the inner surface of the heart (endocardium) or heart valves due to an infection in the bloodstream, usually with bacteria (commonly, streptococci or staphylococci) or fungi
It causes fever, heart murmurs, petechiae, anemia, embolic phenomena, and endocardial vegetations
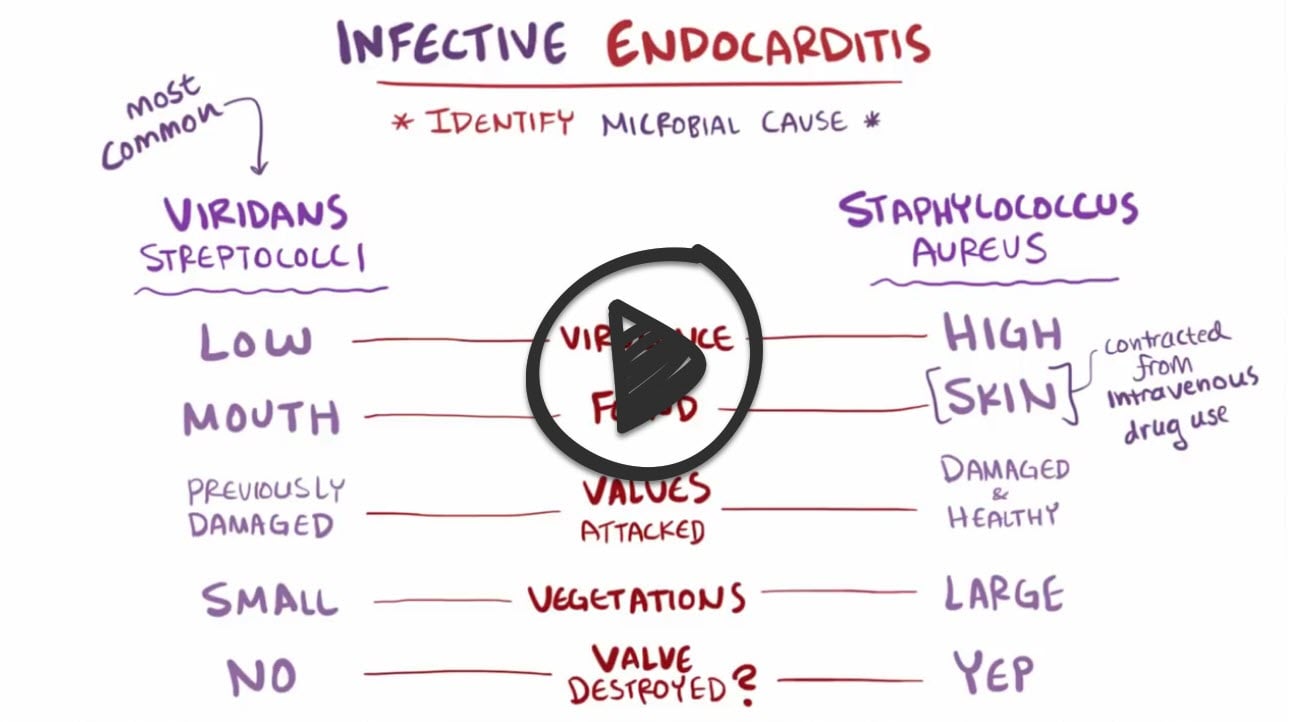
- Acute bacterial endocarditis: Infection of normal valves with a virulent organism (S. aureus)
- Subacute bacterial endocarditis: Indolent infection of abnormal valves with less virulent organisms (S. viridans)
- Endocarditis in intravenous drug users - Staphylococcus aureus
- Prosthetic valve endocarditis - Staphylococcus epidermidis
- Dental procedure, slow onset, damaged valve → Strep viridans (oral flora)

"Always look for the "portal of entry" in the history: Mouth = Viridans; Skin/IVDU = Staph aureus; Genitourinary or gastrointestinal procedures = Enterococcus; Prosthetic valve or intracardiac hardware (biofilm formation)= Staphylococcus epidermidis"
Vegetations may result in valvular incompetence or obstruction, myocardial abscess, or mycotic aneurysm.
- Candida is a slow-growing organism. The most common source is a contaminated line. It typically causes large vegetations in endocarditis.
- Large vegetation endocarditis in the early post–valve replacement period (2 months post-surgery) is most likely due to fungus, that is, Candida infection. Amphotericin B is recommended, followed by several weeks of antifungals that carry fewer adverse events.
- HACEK organisms tend to grow on native valves
- Staphylococcus aureus causes smaller vegetations; it is more common in injection drug users
- Streptococcus viridans is the most common cause of endocarditis. It typically occurs as a late complication of valve replacement and presents as small vegetations and embolic events.
- Endocarditis can occur at any age. Men are affected about twice as often as women. IV drug abusers and immunocompromised patients are at the highest risk.
- Most patients with a new murmur or change in an existing murmur, signs of heart failure (rales, edema) if valve function is compromised
- Janeway lesions: These are small, non-tender, painless bumps on the palms of the hands and soles of the feet. They are caused by emboli (small pieces of bacteria) that lodge in small blood vessels in the skin.
- Osler nodes (remember “O” for “ouchy”: These are tender, painful bumps on the fingertips and toes. They are also caused by emboli that lodge in small blood vessels in the skin.
- Roth spots: These are small, round hemorrhages (bleeding) in the retina. They are caused by emboli that damage the blood vessels in the retina.
- Splinter hemorrhages: These are small, linear hemorrhages under the fingernails or toenails. They are caused by emboli that damage the blood vessels in the nail beds.
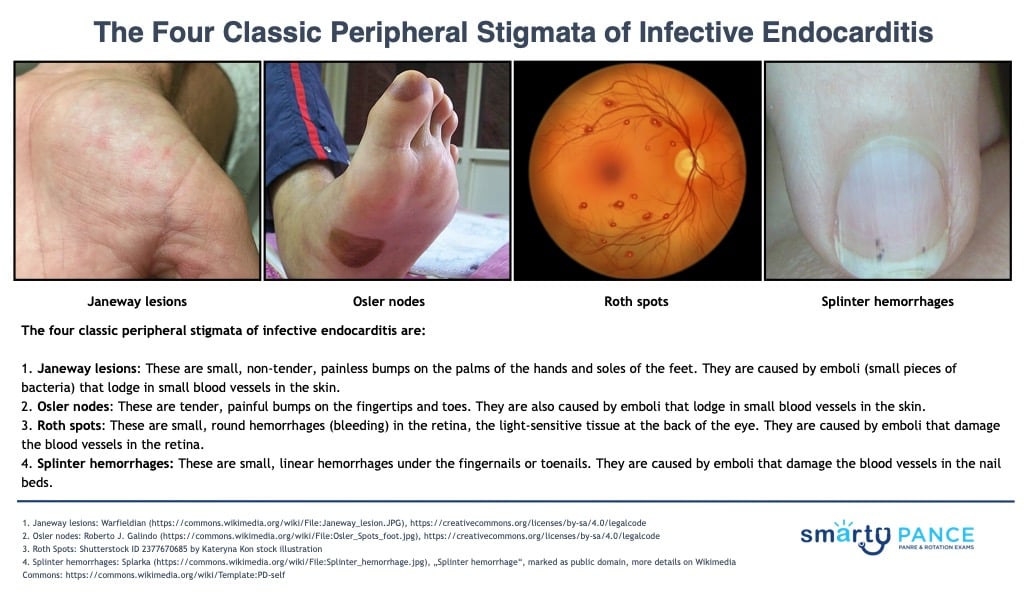
The peripheral stigmata of infective endocarditis are not always present, and they can be seen in other conditions, such as rheumatic fever and systemic lupus erythematosus. However, they can be a valuable clue to the diagnosis of infective endocarditis, especially if they are present in conjunction with other symptoms of the condition, such as fever, chills, and a heart murmur.
In addition to the four classic peripheral stigmata, there are several other physical signs that can be seen in people with infective endocarditis. These include:
- Petechiae: These are small, flat hemorrhages on the skin. They are caused by bleeding from small blood vessels.
- Purpura: These are larger, raised hemorrhages on the skin. They are also caused by bleeding from small blood vessels.
- Clubbing: This is a thickening of the fingertips and/or toenails. It is caused by a decrease in the amount of oxygen in the blood.
- Splenomegaly: This is an enlargement of the spleen. It is caused by an increased number of white blood cells in the spleen.
- Hepatomegaly: This is an enlargement of the liver. It is caused by inflammation or infection of the liver.
- Hematuria: Due to emboli or glomerulonephritis.
- Neurologic findings consistent with CVA, such as visual loss, motor weakness, and aphasia
Rheumatic carditis and infective endocarditis are frequently confused on exams, yet they differ fundamentally in mechanism, timing, and organ involvement. This comparison also includes post-streptococcal glomerulonephritis (PSGN)—another Group A Streptococcus–related condition—to clarify which diseases represent immune-mediated sequelae versus active infection. Viewing these entities side-by-side reinforces the key distinctions PANCE/PANRE questions rely on, including when symptoms occur, whether bacteria are present, and which organ systems are affected.
| Feature | Rheumatic Carditis (ARF) | Post-streptococcal Glomerulonephritis (PSGN) | Infective Carditis (Endocarditis) |
| Causative/trigger organism | ✅ Group A Streptococcus (GAS) (Streptococcus pyogenes) | ✅ Group A Streptococcus (GAS) (Streptococcus pyogenes) | ❌ Most commonly Staph aureus, Strep viridans |
| Role of GAS | Triggers autoimmune reaction | Triggers immune-complex disease | Rare cause |
| Mechanism | Molecular mimicry → inflammation | Immune-complex deposition | Direct bacterial infection |
| Active infection at presentation? | ❌ No | ❌ No | ✅ Yes |
| Timing after strep infection | 2–4 weeks | 1–3 weeks | Days–weeks (during bacteremia) |
| Primary organ affected | Heart | Kidneys | Heart valves |
| Blood cultures | Negative | Negative | Positive |
| Key pathology | Valvular inflammation → regurgitation | Glomerular inflammation → hematuria | Vegetations ± valve destruction |
| Typical murmur | ✅ New mitral regurgitation | None | ✅ New or changing regurgitant murmur |
| Urinalysis findings | Normal | Hematuria, proteinuria | Usually normal |
| Complement levels | Normal | Low C3 | Normal |
| Does treating strep prevent it? | Yes | No | N/A |
| Long-term sequelae | Chronic rheumatic heart disease | Usually resolves (rare CKD) | Heart failure, emboli |
Diagnosis requires demonstration of microorganisms in blood and usually echocardiography
- Blood cultures (before antibiotics are started) 3 sets at least 1 hour apart
- EKG at regular intervals
- LABS: CBC, ESR, RF
A transesophageal echocardiogram is the gold standard
Modified Duke Criteria for Diagnosis of Infectious Endocarditis
Definite: 2 major criteria, or 1 major and 3 minor criteria, or 5 minor criteria
Possible: 1 major and 1 minor criteria, or 3 minor criteria
- Major clinical criteria
- Positive blood culture: isolation of typical microorganism for IE from 2 separate blood cultures or persistently positive blood culture
- Single positive blood culture for C. burnetii or antiphase-1 IgG antibody titer >1:800
- Positive echocardiogram: presence of vegetation, abscess, or new partial dehiscence of a prosthetic valve; must be performed rapidly if IE is suspected
- New valvular regurgitation (change in preexisting murmur not sufficient)
- Minor criteria
- Predisposing heart condition or IV drug use
- Fever ≥38.0°C (100.4°F)
- Vascular phenomena: major arterial emboli, septic pulmonary infarcts, mycotic aneurysm, intracranial hemorrhage, conjunctival hemorrhage, Janeway lesions
- Immunologic phenomena: glomerulonephritis, Osler nodes, Roth spots, rheumatoid factor (RF). Microbiologic evidence: positive blood culture, but not a major criterion (excluding single positive cultures for coagulase-negative staphylococci and organisms that do not cause endocarditis) or serologic evidence of infection likely to cause IE
Management – treatment consists of prolonged IV antibiotics and sometimes surgery
- IV antibiotics tailored to organism and susceptibility
- Valve debridement, repair, or replacement if indicated
- Start empiric therapy after obtaining 3 sets of blood cultures
- Empiric therapy includes vancomycin + Ceftriaxone (covers MRSA, MSSA, Strep, Enterococcus)
- Patients with a prosthetic valve receive IC vancomycin + Cefepime + Rifampin ± Gentamicin
- IV drug users receive vancomycin (to cover MRSA)
- Use vancomycin in penicillin-allergic patients
Antibiotic prophylaxis (only for high-risk patients)
- Amoxicillin 2 g PO 30–60 minutes before procedure
- Penicillin allergy: Cephalexin 2 g PO, Azithromycin/clarithromycin 500 mg PO or doxycycline 100 mg PO
 Osmosis Osmosis |
|
 |
Bacterial endocarditis is an infection of the inner surface of the heart or heart valves due to bacteria in the bloodstream, typically introduced via dental or medical procedures in the mouth, intestinal tract, or urinary tract. The bacteria can grow on the edges of a heart defect or surface of an abnormal valve and continue to grow to produce large particles called vegetations. These particles can then break off and embolize to the lungs, brain, kidneys, and skin. Symptoms and signs of endocarditis vary but include prolonged fever, a new or changing heart murmur, and specific vascular and immunologic phenomena. Vascular phenomena include septic emboli, Janeway lesions, splinter hemorrhages, and renal and splenic infarcts. Immunologic phenomena include Osler’s nodes and Roth’s spots.
Play Video + QuizDuke’s Criteria

The Duke criteria are a set of clinical criteria set forward for the diagnosis of infective endocarditis. Fulfilling the criteria includes either having 2 major criteria, 1 major and 3 minor criteria, or 5 minor criteria. The two major criteria are positive blood cultures for infective endocarditis and evidence of endocardial involvement. The five minor criteria are having a predisposing heart condition or intravenous drug use, fever, vascular phenomena, or having microbiologic evidence or echocardiographic evidence that does not meet the major criteria.
Play Video + QuizQuestion 1 |
True | |
False |
Question 2 |
True | |
False |
Question 3 |
True | |
False |
Question 4 |
True | |
False |
Question 5 |
Bicuspid aortic valve | |
Prosthetic heart valve | |
Congenital heart disease | |
History of endocarditis |
Question 6 |
Amoxicillin 2g 30-60 minutes before the procedure | |
Amoxicillin 1g 30-60 minutes before the procedure | |
Amoxicillin 2g three hours before the procedure | |
Clindamycin 600 mg 30-60 minutes before the procedure |
Question 7 |
Fever greater than 100.4 | |
Sustained bacteremia (2 + blood cultures by organism known to cause endocarditis) | |
Predisposing condition (abnormal valves, IVDA, indwelling catheters) | |
Immunologic phenomena: Osler's nodes, Roth spots | |
Vascular and Embolic phenomena: Janeway lesions, pulmonary emboli |
Question 8 |
Candida albicans | |
HACEK organisms Hint: HACEK organisms tend to grow on native valves. | |
Staphylococcus aureus Hint: Staphylococcus causes smaller vegetations; it is more common in injection drug users. | |
Streptococcus viridans Hint: Streptococcus viridans is the most common cause of endocarditis. It typically occurs as late complication of valve replacement and presents as small vegetations and embolic events. |
Question 9 |
Electrocardiogram Hint: This patient's signs and symptoms are consistent with infective endocarditis. The diagnostic study of choice would be a transesophageal echocardiogram. | |
CT angiogram of the chest Hint: This patient's signs and symptoms are consistent with infective endocarditis. The diagnostic study of choice would be a transesophageal echocardiogram. | |
Cardiac catheterization Hint: This patient's signs and symptoms are consistent with infective endocarditis. The diagnostic study of choice would be a transesophageal echocardiogram. | |
Transesophageal echocardiogram |
Question 10 |
This patient does not require antibiotic prophylaxis for a routine dental cleaning. | |
This should receive Pen VK 250 mg p.o. QID for 10 days after the procedure. | |
This patient should receive Amoxicillin 2 grams 30-60 minutes before the procedure Hint: This would be the preferred regimen for a patient requiring antibiotic prophylaxis. See A for explanation. | |
This patient should receive Erythromycin 250 mg QID for 1 day before the procedure and then 10 days after the procedure. |
Question 11 |
Metabolic acidosis Hint: See B for explanation. | |
Systemic arterial embolization of vegetation | |
Hypotension and tachycardia Hint: See B for explanation. | |
Activation of the immune system Hint: Glomerulonephritis and arthritis result from activation of the immune system. |
Question 12 |
Acute myocardial infarction Hint: Acute MI presents with complaint of chest pain, SOB, not with fever and myalgias. | |
Bacterial endocarditis | |
Acute pericarditis Hint: Pericarditis does not present with systolic or diastolic murmur or vegetation, more commonly pericardial friction rub would be noted. | |
Restrictive cardiomyopathy Hint: Restrictive cardiomyopathy will show impaired diastolic filling on echocardiogram and is not associated with fever. |
|
List |
References: Merck Manual · UpToDate