Depressive disorders
| Major depressive disorder | A mood disorder in which a person experiences, in the absence of drugs or a medical condition, two or more weeks of significantly depressed moods, feelings of worthlessness, and diminished interest or pleasure in most activities. |
| Persistent depressive disorder (dysthymia) | Mood disorder involving persistently depressed mood, with low self-esteem, withdrawal, pessimism, or despair, present for at least 2 years, with no absence of symptoms for more than 2 months. |
| Premenstrual dysphoric disorder | A disorder marked by repeated episodes of significant depression and related symptoms during the week before menstruation |
| Suicidal/homicidal behaviors | Mood disturbances, somatic complaints, feeling hopelessness, worthlessness, helplessness |
| Major depressive disorder | a 33-year-old woman complaining of fatigue and decreased interest in “the things that used to make me happy.” She is sleeping less and eating less, and she says that she is forcing herself to eat “because I know I have to eat something.” She finds herself spending less time with her kids and husband as she retreats to her room. She feels guilty that she lacks the energy and enthusiasm she used to have. 5 or more SIEGECAPS for≥ 2 weeks nearly every day and at least one of the symptoms is depressed mood or anhedonia SIGECAPS:
Treatment: SSRIs are the first line treatment
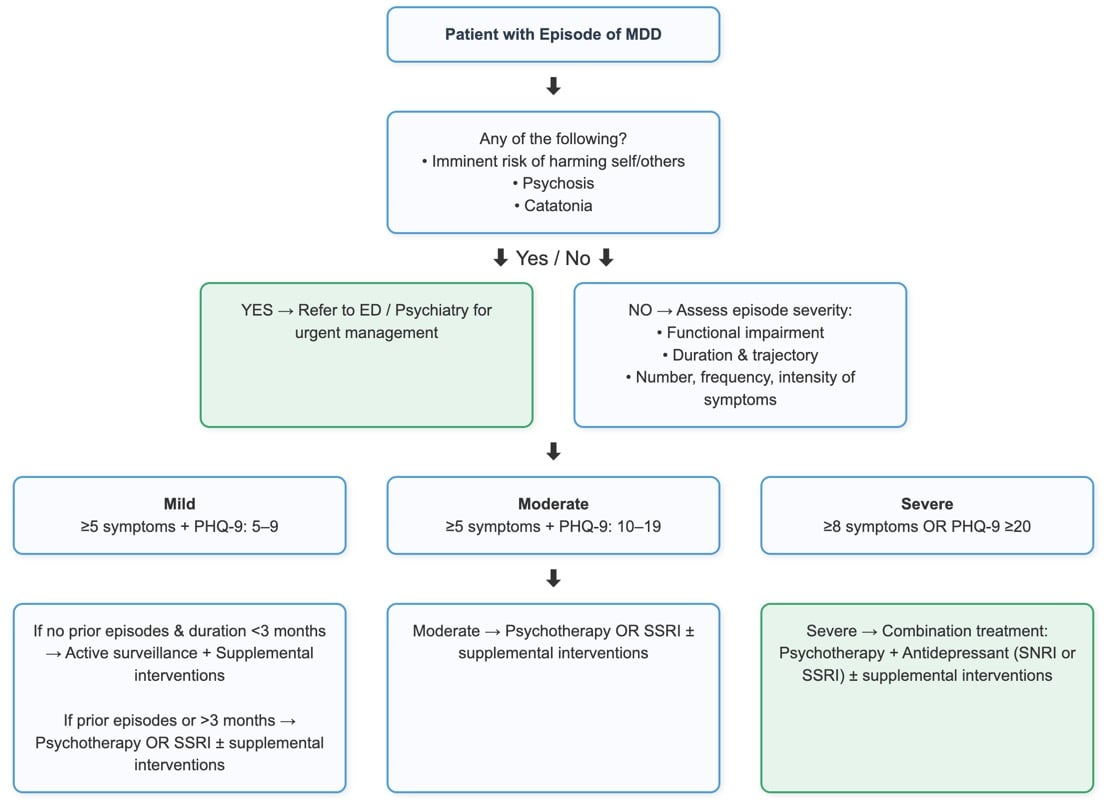 Adapted from UpToDate |
| Persistent depressive disorder (dysthymia) | Patient will present as → a 30-year-old married male who feels down most of the time for the past three years. He experiences frequent, intrusive thoughts that he is not good enough, despite personal and professional successes. He tries to overcompensate for his thoughts by taking on more than he can handle, which leads to failure and furthers his feelings of inadequacy. His wife suggests that he seek help after finding him crying. A patient with chronic depression for two years or more Chronic depressions - depressive symptoms for > 2 years
Treatment:
|
| Premenstrual dysphoric disorder | Patient will present as → a 26-year-old patient is complaining of depression and anxiety just prior to her menses. The symptoms have been going on for more than 1 year, but are now starting to interfere with her relationships and her productivity at work. One week prior to menses each month she experiences a depressed mood, a feeling of being on edge, increased irritability, difficulty sleeping, a feeling of being overwhelmed, and is easily fatigued. She charted her symptoms daily in a log and returned to the office two cycles later. The log is consistent with the history. Her physical examination and general laboratory profile showed no abnormalities. Repeated episodes of significant depression and related symptoms during the week before menstruation In the majority of menstrual cycles, at least five symptoms must be present in the final week before the onset of menses, start to improve within a few days after the onset of menses, and become minimal or absent in the week post menses. One (or more) of the following symptoms must be present:
One (or more) of the following symptoms must additionally be present, to reach a total of five symptoms when combined with symptoms from above.
Treatment: SSRIs are first-line treatment (fluoxetine, sertraline, paroxetine, escitalopram) and can be used continuously or instituted the week prior to menses.
|
| Suicidal/homicidal behaviors | Patient will present as → a 17-year-old female who attempts suicide by swallowing several tablets of acetaminophen. Suicide is the 8th leading cause of death in the United States and the 3rd leading cause of death in ages 15-24 years.
Assess level of intent, level of lethality, risk factors:
Consider referral to emergency services
|