| DSM-5 Trauma and Stressor-Related Disorders
Items in bold are covered as part of the NCCPA PANCE/PANRE Psychiatry Blueprint and will be covered here. Additional topics may be covered in the PAEA EOR™ Psychiatry Topic List. |
|
|
|
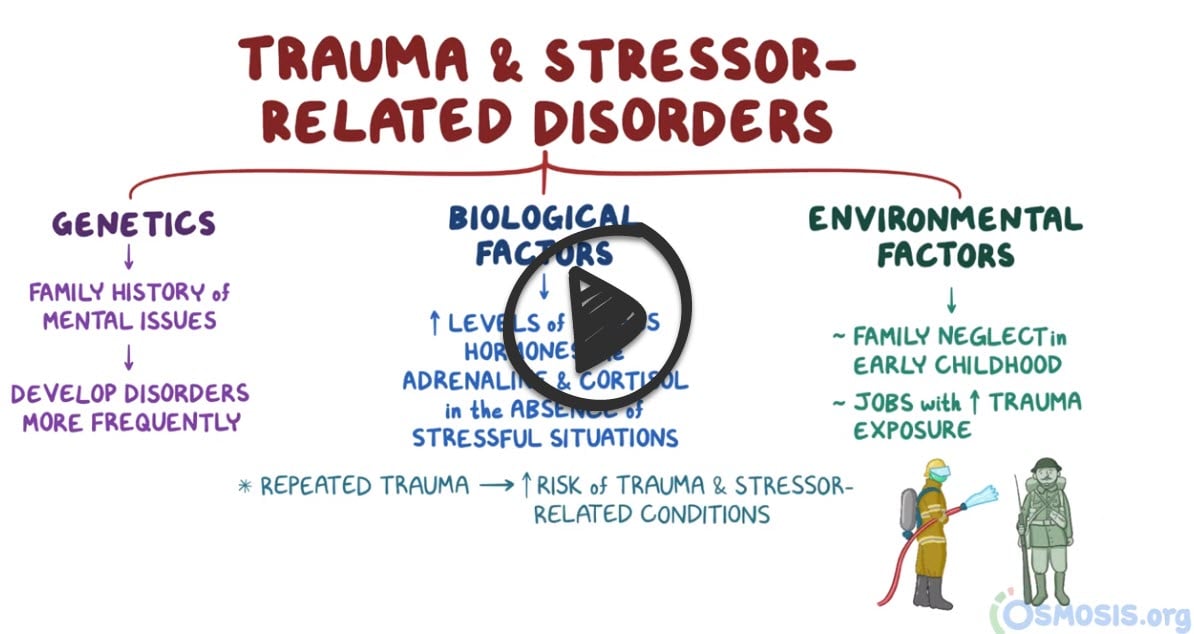
Trauma and stressor-related disorders
 |
|
| Adjustment disorders | Prolonged negative emotional reaction following a major life stressor (e.g., divorce, moving, new job) |
| Post-traumatic stress disorder | An anxiety disorder characterized by haunting memories, nightmares, social withdrawal, jumpy anxiety, and/or insomnia that lingers for four weeks or more after a traumatic experience |
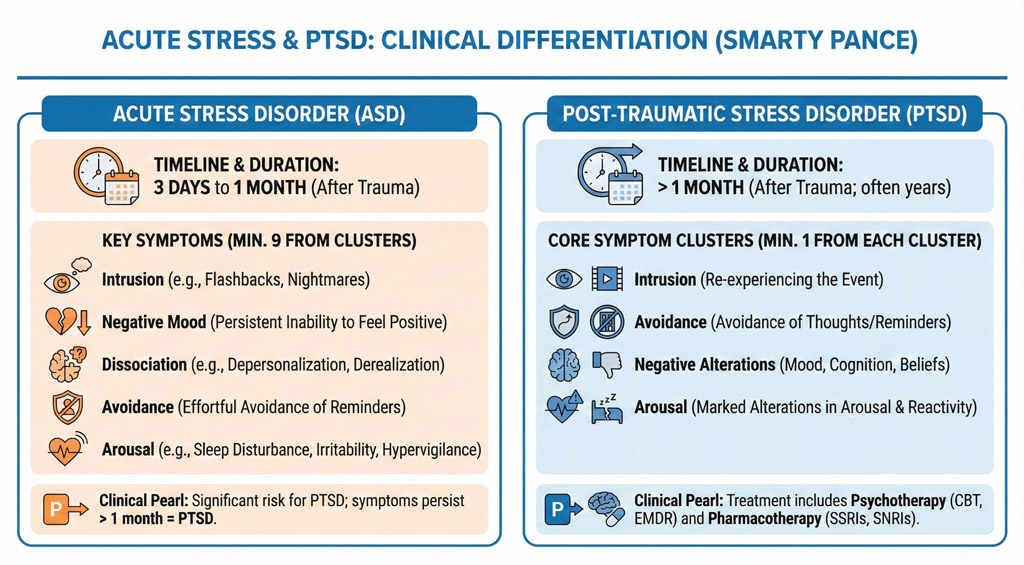
| Acute stress disorder (ASD) | Acute stress disorder is a period of intrusive recollections that occurs after witnessing or experiencing a traumatic event. ASD occurs within one month of the traumatic event and lasts from three days up to one month |
| Acute stress disorder (PANRE) (ASD) | Patient will present as → a 25-year-old individual who was involved in a severe car accident three weeks ago. They report experiencing recurrent, involuntary, and intrusive distressing memories of the car accident. They have been feeling on edge, have difficulty sleeping, and actively avoid reminders of the accident. They also feel detached from others and lose interest in activities they used to enjoy. The patient is diagnosed with acute stress disorder. Management includes trauma-focused cognitive behavioral therapy, with SSRIs considered if symptoms are severe. Close follow-up is recommended to assess for resolution or progression to PTSD.
Acute Stress Disorder (ASD) is characterized by the development of severe anxiety, dissociation, and other symptoms that occur within one month after exposure to an extreme traumatic stressor PTSD vs. ASD
Acute stress disorder is a period of intrusive recollections that occurs after witnessing or experiencing a traumatic event. The characteristics of this disorder differ from those of posttraumatic stress disorder in that ASD occurs within one month of the traumatic event and lasts from three days up to one month, whereas PTSD symptoms must last more than one month. DX: Diagnosis is based on clinical criteria from the DSM-5, which requires the presence of nine or more symptoms from any of the five categories of intrusion, negative mood, dissociation, avoidance, and arousal, beginning or worsening after the traumatic event and lasting for three days to one month TX: Early intervention is crucial. Cognitive Behavioral Therapy (CBT), specifically Trauma-focused cognitive-behavioral therapy (TF-CBT), is the most effective treatment for ASD
|
| Adjustment disorders | Patient will present as → a 35-year-old female presents with sadness, irritability, and difficulty concentrating for two months following the unexpected loss of her job. She reports worry about her financial future and withdrawal from friends, but denies suicidal thoughts or prior mental health issues. Examination reveals a tearful individual with an anxious mood. Symptoms began within three months of the stressor and do not meet criteria for major depression. She is diagnosed with adjustment disorder with mixed anxiety and depressed mood. Management includes cognitive behavioral therapy (CBT) and supportive care, with a follow-up scheduled to monitor progress. Adjustment Disorders are the disproportionate response to a stressor that would typically be expected (ex., job loss, physical illness), which begin within 3 months of the stressor and end within 6 months after the stressor resolved
DX: Diagnosis requires:
Differential diagnosis includes major depressive disorder (MDD), generalized anxiety disorder (GAD), and post-traumatic stress disorder (PTSD); adjustment disorders are directly linked to a stressor and are typically less severe TX: Psychotherapy is the treatment of choice, focusing on stress management and coping strategies (e.g., cognitive-behavioral therapy)
|
| Bereavement and Grief Reaction | Patient will present as → a 42-year-old female presents with intense sadness, loss of appetite, and difficulty sleeping following the death of her husband three weeks ago. She reports crying frequently and feeling guilty, but denies thoughts of self-harm. Despite her grief, she continues to care for her children and perform daily tasks. Examination reveals a tearful but alert individual with appropriate affect. Screening for depression is negative. She is diagnosed with bereavement and provided psychological support. Referral to grief counseling is offered, and she is educated on signs of complicated grief. Follow-up is scheduled to monitor her progress. Bereavement and Grief Reaction are normal responses to the loss of a loved one, characterized by emotional, cognitive, and physical reactions, which may progress to pathological grief in some cases.
|
| Post-traumatic stress disorder (PTSD) | Patient will present as → 33-year-old male presents with difficulty sleeping. The patient states that these symptoms began approximately 3 months ago when he lost his close friend while they were both in combat. He re-experiences this loss during the day and in his dreams. The patient reports anxiety and depression. The patient has experienced a traumatic event that causes an acute stress reaction. Once the symptoms persist past 1 month it is now considered post-traumatic stress disorder (PTSD) Treatment: SSRIs are considered first-line along with cognitive-behavioral therapy (CBT)
|