


15 y/o with a non-pruritic, blanching rash
Patient will present as → a 15-year-old complaining of several red lesions on her palms, the back of her hands, and on her lips for one-week duration. On examination, you note a symmetrical red papular rash with many target lesions. The rash appeared just a few days after herpes facialis.
Erythema multiforme (EM) is an acute, immune-mediated (type IV hypersensitivity) reaction most often triggered by infections (especially HSV and Mycoplasma pneumoniae); less commonly by drugs (sulfonamides, β-lactams, antiepileptics)
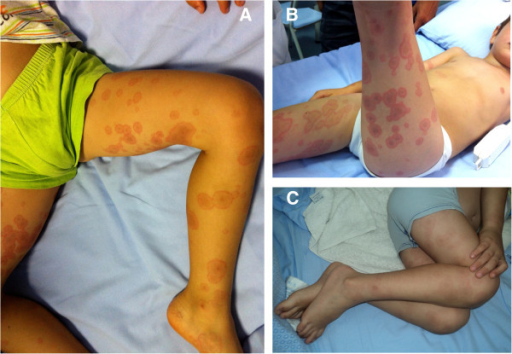
- Skin lesions predominantly involving the extremities (hands, feet, and mucosa)
- Target-like shape, raised, blanching, and lack of itchiness help characterize this rash
- Divided into erythema multiforme (EM) major and minor and is now regarded as distinct from Stevens-Johnson Syndrome (SJS) and Toxic Epidermal Necrolysis (TEN), which is a more severe mucocutaneous reaction that is usually caused by a medication
- EM minor – Target lesions limited to skin; mucosal involvement absent or mild (usually oral only); patients otherwise well.
-
- EM major – Widespread skin lesions with significant mucosal involvement (≥1 site – oral, ocular, or genital); may include systemic symptoms (fever, malaise, arthralgias).
Causes: Infections are associated with at least 90% of cases of erythema multiforme - most commonly HSV
- Most common = infection, Herpes simplex, Mycoplasma pneumoniae important in children, upper respiratory infections. Less common = drugs (e.g., sulfonamides, β-lactams, phenytoin). Often idiopathic.

"EM may appear similar to Steven Johnson Syndrome (SJS) but SJS has a more generalized distribution of lesions; concentrated on the trunk (EM extremities and mouth), an absence of raised typical target lesions and atypical flat (not raised) target lesions or macules with the coalescence of lesions."
Diagnosis is based on absent or mild prodromal symptoms, preceding HSV infection (up to 50% of cases) 10–15 days before the skin eruptions and a rash involving the skin and sometimes the mucous membrane, most commonly the mouth.
Presents as raised (papular), target lesions with multiple rings and dusky center (as opposed to annular lesions in urticaria)
- Three concentric zones of color from center to outer ring
- central dusky/dark area that can be crust or vesicle
- paler pink or edematous zone
- peripheral red/dark ring
- Fixed lesions (as opposed to urticaria, in which lesions typically resolve within 24 hours)
- Negative Nikolsky sign (as opposed to SJS/TEN)
- Generally mild burning or itchiness; nontender
- Most commonly involves
- palms/soles
- backs of hands and feet
- extensor aspects of forearms and legs
- Must also examine mucosal surfaces and eyes
- oral
- genital/anal
- iris
Symptomatic treatment with oral antihistamines and topical corticosteroids for mild cases; mouthwashes or topical steroid gels for oral disease.
EM major (involvement of mucous membranes and systemic signs)
- Corticosteroids
- Ophthalmology consult if ocular involvement
EM minor (no mucous membrane involvement and no systemic signs) is usually self-limited
- Supportive care
Early treatment with acyclovir may lessen the number and duration of cutaneous lesions for patients with coexisting or recent HSV infection.
- Acyclovir for adults: 200 mg, 5× a day for 7–10 days in the onset of EM
- For pediatric patients: 10 mg/kg/dose TID for 7–10 days
Erythema multiforme

Grook Da Oger, CC BY-SA 3.0, via Wikimedia Commons
{kind=link}
 Osmosis Osmosis |
|
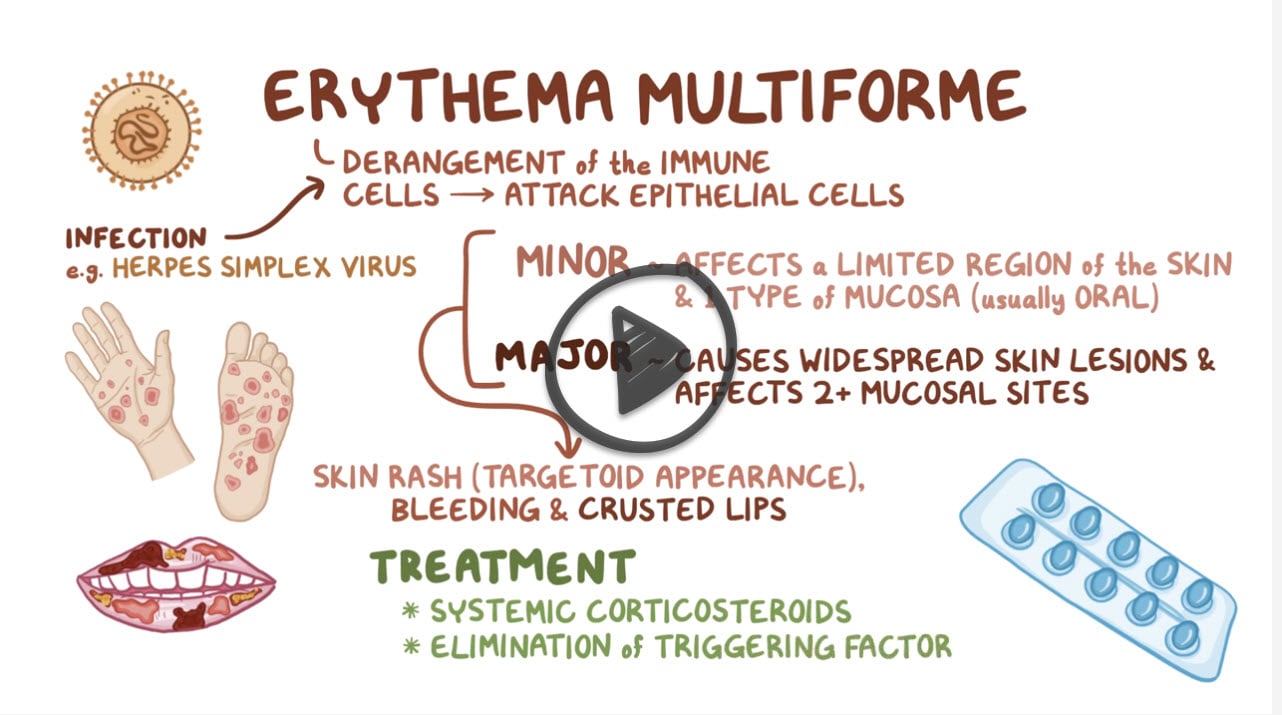 |

Erythema multiforme (EM) is an acute, immune-mediated. and sometimes recurring skin condition that is considered to be a type IV hypersensitivity reaction. It is associated with some infections such as HSV or Mycoplasma pneumoniae, or less frequently medications. The presence of EM is characterized by the appearance of distinctive target-like lesions on the skin in a symmetrical distribution. Mild symptoms is classified as EM minor while mucosal involvement is classified as EM major. The disease is self-limiting but topical ointments may provide symptomatic relief.
Play Video + QuizQuestion 1 |
Dome-shaped, waxy, umbilicated papules Hint: Describes Molluscum contagiosum | |
Silvery scales on well-demarcated erythematous plaques Hint: Psoriasis | |
Pruritic coin-shaped plaques or grouped vesicles with an erythematous base typically occurring during the cold seasons Hint: Nummular eczema | |
Target lesion with variable mucous membrane involvement | |
Tender nodules and bullae Hint: Seen with conditions like bullous pemphigoid |
Question 2 |
Autoimmune collagen vascular disease Hint: This is more commonly associated with conditions like lupus, not erythema multiforme. | |
Drug hypersensitivity reaction Hint: While drugs can cause erythema multiforme, the recent HSV infection in this case points more towards an infection-triggered cause. | |
Infection-triggered immune response | |
Genetic predisposition to skin malignancies Hint: There is no direct association between erythema multiforme and genetic skin malignancies. | |
Chronic exposure to ultraviolet radiation Hint: UV radiation is not a primary cause of erythema multiforme. |
Question 3 |
Skin biopsy for histopathology Hint: Biopsy is rarely needed to confirm the diagnosis | |
Direct immunofluorescence (DIF) of perilesional skin Hint: Not indicated to make the diagnosis | |
Tzanck smear of lesion scrapings Hint: Used for viral infections but not useful for EM diagnosis | |
Patch testing for causative antigens Hint: Helps identify triggers but not required or specific for diagnosing EM | |
Clinical evaluation alone |
Question 4 |
Systemic corticosteroids Hint: Generally reserved for more severe cases or erythema multiforme major. | |
Antiviral therapy | |
High-potency topical corticosteroids Hint: May provide symptomatic relief but are not the primary treatment in HSV-associated cases, especially in thi case of recurrent EM. | |
Oral antibiotics Hint: Indicated if there is a secondary bacterial infection, which is not suggested in this scenario. | |
Phototherapy Hint: Not a standard treatment for erythema multiforme. |
|
List |
References: Merck Manual · UpToDate