The NCCPA™ PANCE Dermatology Content Blueprint covers three dermatologic bacterial infections
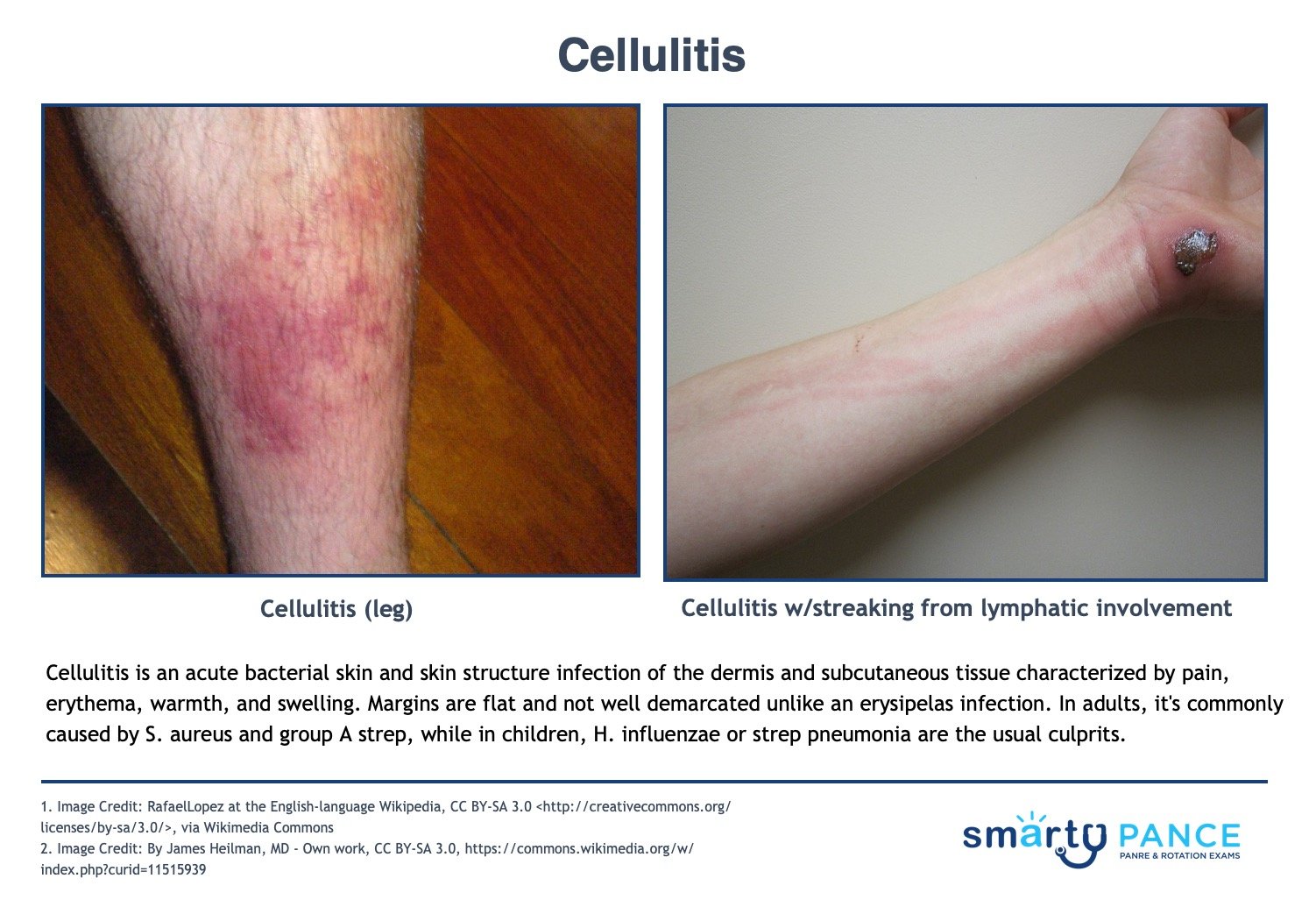
| Cellulitis (ReelDx) | ReelDx Virtual Rounds (Cellulitis)Patient will present as → a 64-year-old female with a 4 cm × 7 cm edematous, red, hot tender area on the left thigh. The lesion has gotten larger over the past 6 hours. She tells you she has also had a low-grade fever and some chills. On physical exam, there is a poorly demarcated 12cm red and tender plaque on her right calf. Some parts resemble an orange peel. There is a superficial cut in the middle of the plaque. An acute bacterial skin and skin structure infection of the dermis and subcutaneous tissue; characterized by pain, erythema, warmth, and swelling. Margins are flat and not well demarcated.
DX: Culture should be taken of all purulent wounds and followed up in 48 hours Treat mild cellulitis (MSSA)
Cat bites with augmentin or doxycycline if PCN allergic
Treat purulent or methicillin-resistant Staphylococcus aureus infection (MRSA) with
View more images of cellulitis |
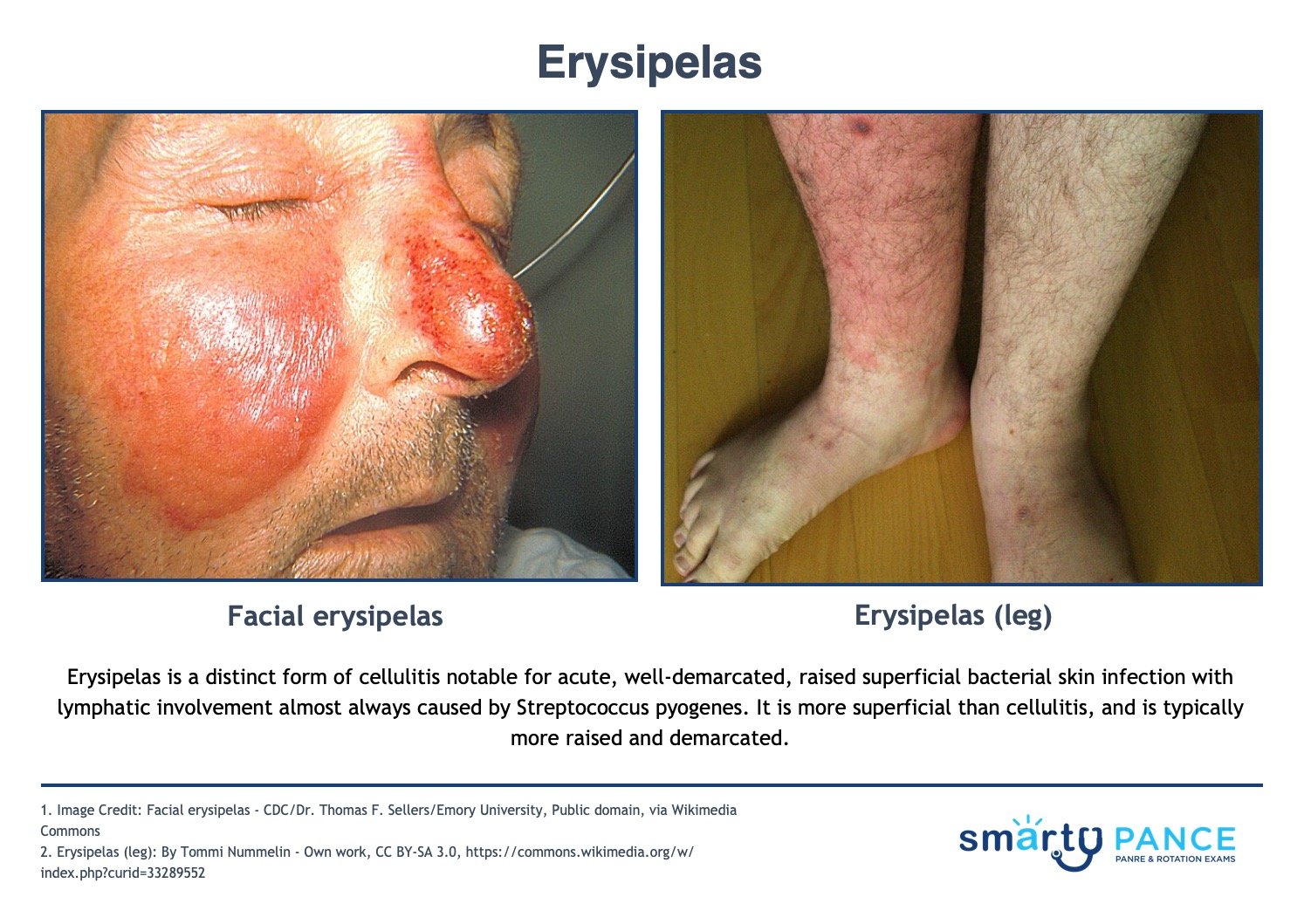
| Erysipelas | Patient will present as → a 19-year-old female with a painful rash on her left leg. She had a small bug bite in the same area about three weeks ago. Since then, the area has become red, painful, and hot. On physical exam, you note shiny, raised, indurated, and tender plaque-like lesions on the left leg. The redness is well-demarcated and hot to the touch. You send her home on penicillin. A distinct form of cellulitis notable for acute, well-demarcated, raised superficial bacterial skin infection with lymphatic involvement almost always caused by Streptococcus pyogenes
DX: Wound culture and sensitivity
TX: Treat with antibiotics: regimen depends on location and severity
View more images of erysipelas |
| Impetigo | ReelDx Virtual Rounds (Impetigo)Patient will present as → a 5-year-old girl with crusting facial lesions present for 3 days. The mother reports that prior to the development of the facial lesions, her daughter was scratching at insect bites. Examination reveals a red facial rash with a golden “honey-colored crust” and pruritus. Child < 6 y/o complaining of non-painful, pruritic lesions on the face
Nonbullous impetigo: the most common form of impetigo caused by staphylococcus aureus or streptococcus pyogenes characterized by honey-colored crusts on the face and extremities
Bullous impetigo: staphylococcus aureus impetigo that progresses rapidly from small to large flaccid bullae (newborns/young children) caused by epidermolytic toxin release. There is less lymphadenopathy and the trunk is more often affected; < 30% of patients
DX: The diagnosis is usually made clinically, but rarely a culture may be useful TX: topical mupirocin, dicloxacillin, cephalexin for more severe illness
|