The NCCPA™ PANCE Dermatology Content Blueprint covers three dermatologic conditions under the category of exanthems
 Picmonic
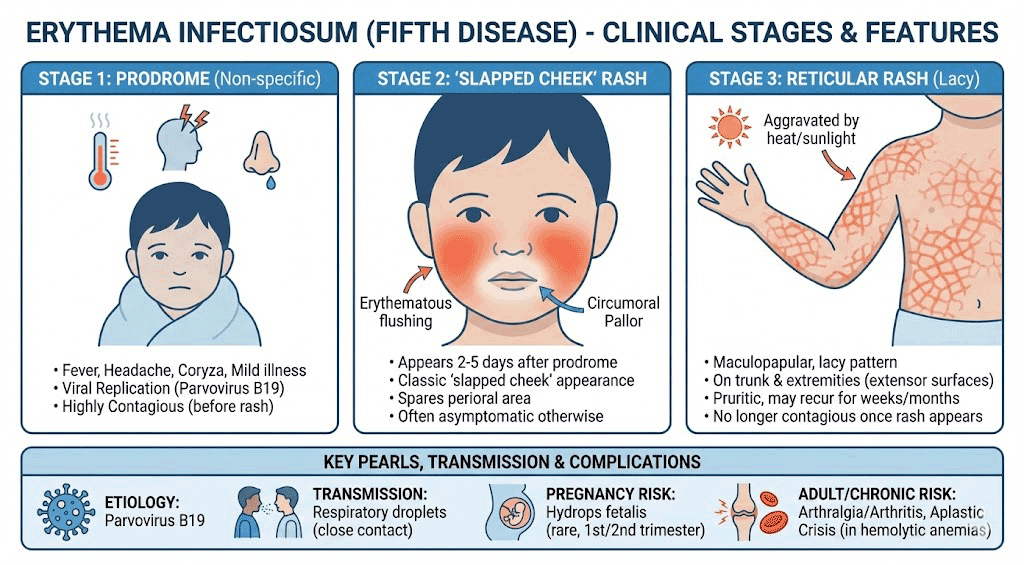
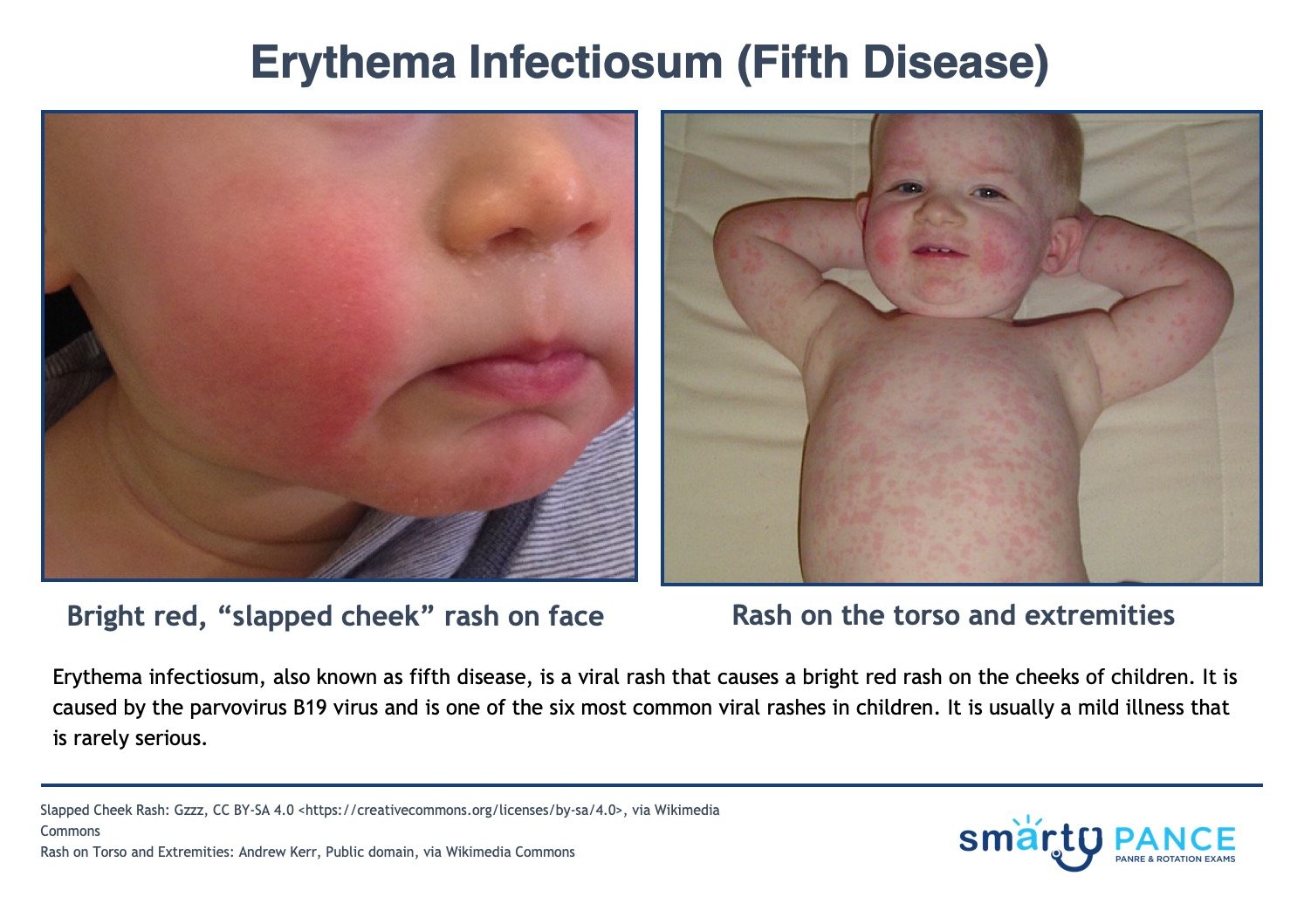
Picmonic| Erythema infectiosum (fifth disease) | ReelDx Virtual Rounds (Erythema infectiosum)Patient will present as → a 4-year-old who is brought to the office by his mother. The child has had a low-grade fever, headache, and sore throat for the past week. Four days ago, he suddenly developed a bright red rash on his cheeks, which during the past two days has spread to the trunk, arms, and legs. On physical examination, the child has erythema of the cheeks and a maculopapular rash with central clearing on the trunk spreading to the extremities. There are no other significant findings.
Erythema infectiosum (also known as Fifth's disease) is a common viral exanthem observed in pediatric patients caused by parvovirus B19
DX: is based primarily on clinical observations, history, and physical exam
TX: Treatment is symptomatic
View more images of erythema infectiosum |
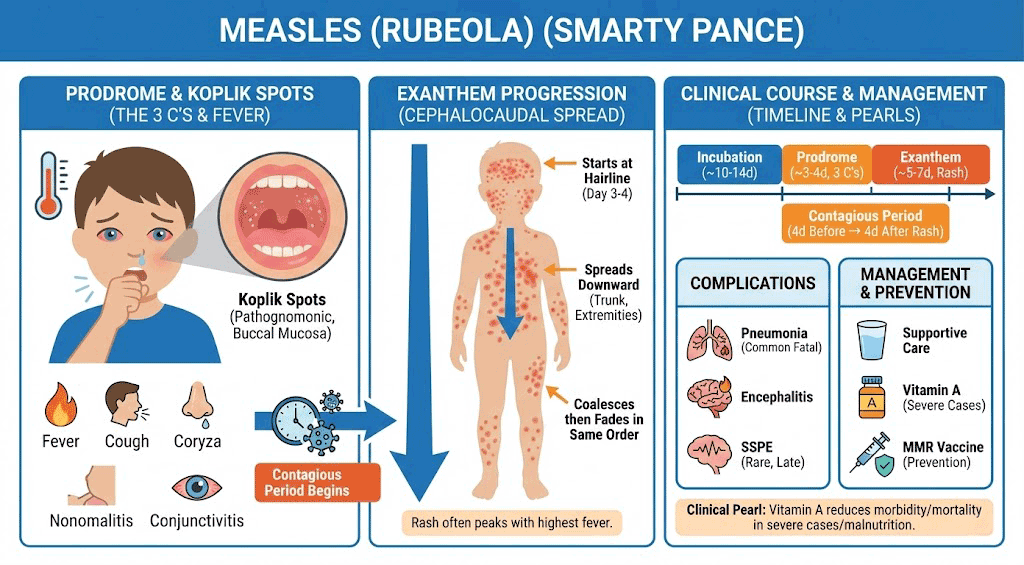
| Measles (Rubeola) | Patient will present as → a 6-year-old child who is brought to the emergency room for a complaint of high fevers and a rash. His mother reports that she thought he had “just a cold” approximately one week ago—he had a mild fever, runny nose, conjunctivitis, and cough. Then, he developed a rash that started on his face and gradually spread downward. The child has no significant past medical history, however, he was adopted from Russia at age 5, and his medical history prior to adoption is unknown. On examination, the child appears lethargic and has a temperature of 104.3. There is a mild injection of his conjunctiva and a generalized macular rash. White macules are noted on his buccal mucosa.
The 4 C's - c ough, c oryza, c onjunctivitis, and c ephalocaudal spread Measles (Rubeola) is caused by a paramyxovirus and is transmitted by respiratory droplets, it has a 10-12 day incubation period. It progresses in three phases characterized by a prodrome, enanthem, and exanthem
DX: Clinical diagnosis of measles requires a history of fever of at least three days, with at least one of the three C's (cough, coryza, conjunctivitis)
TX: Treatment is supportive - anti-inflammatories, isolate for 1 week after onset of rash
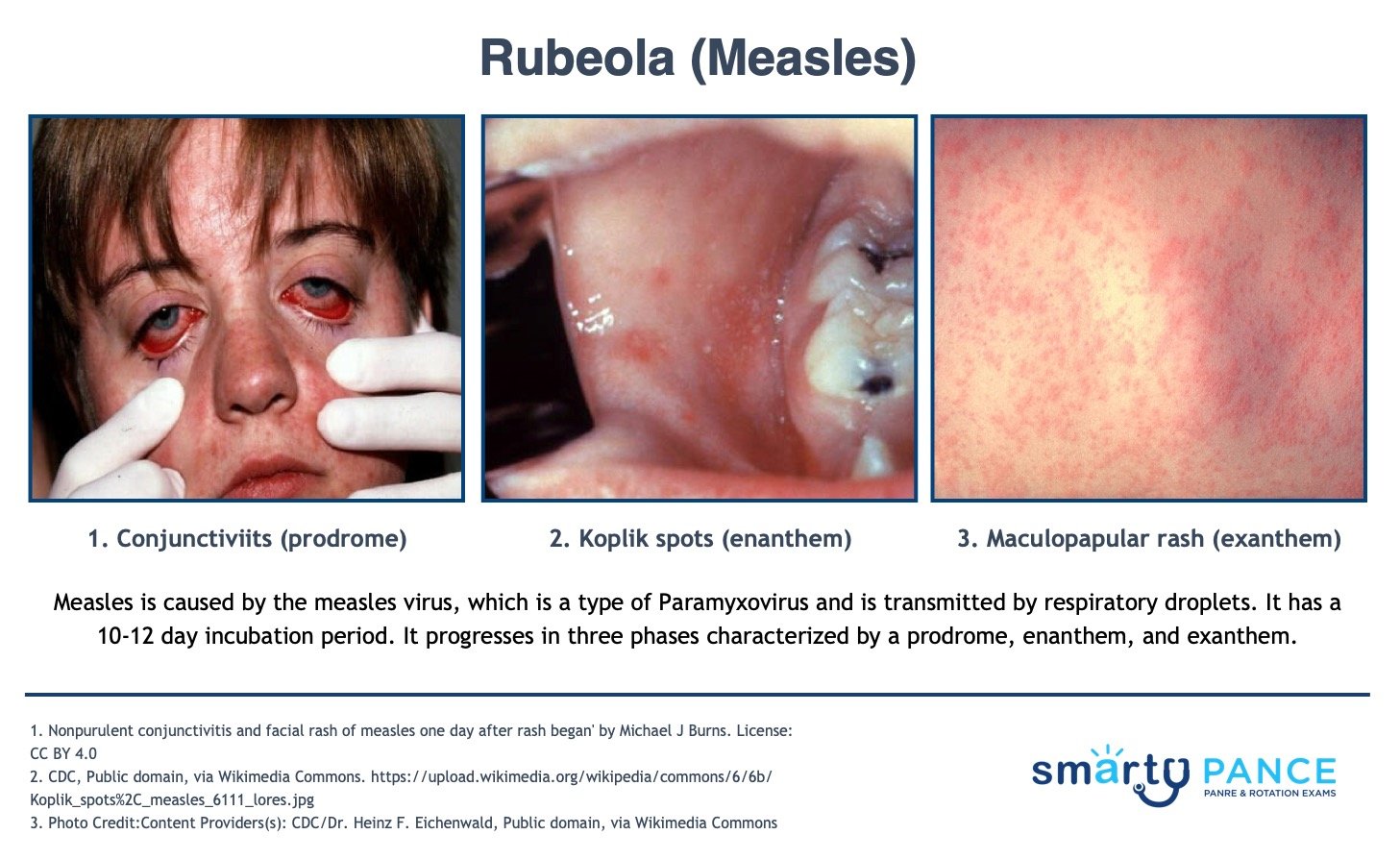
View more images of Rubeola (Measles) |

{kind=link}
{kind=link}
{kind=link}

Roseola is a common exanthem in young children that presents with a high fever followed by a rash. It is usually caused by Human Herpesvirus 6 (HHV-6), which is an enveloped linear double-stranded DNA virus. Children will have 3-5 days of a high fever, which may exceed 40C or 104F, causing some children to develop febrile seizures. Following this, a diffuse macular rash starts on the trunk and spreads to the face and extremities.
Play Video + QuizRubeola (Measles)

Rubeola virus is a single-stranded RNA paramyxovirus that causes measles. Measles is an exanthem that is distinguished by a fever, Koplik spots, cough, coryza (head cold), conjunctivitis and a characteristic rash. Koplik spots are pathognomonic for measles and present as small red spots with a blue-white center on the buccal mucosa. They usually appear during the prodrome phase or about 48 hours before a rash. The rash found in measles is an erythematous maculopapular rash that begins on the face and moves down to involve the entire body, much like the rash in rubella. However, in measles, the rash darkens over time and is confluent (the rash merges together). A rare but fatal complication of measles is subacute sclerosing panencephalitis, which can occur 7-10 years post-infection and is thought to be caused by persistent measles infection in the CNS. In immunocompromised patients, measles can cause pneumonia with Warthin-Finkeldey multinucleated giant cells. Children in the United States are typically vaccinated against measles; however, outbreaks are seen in under-vaccinated or unvaccinated children.
Play Video + QuizCoxsackievirus
Coxsackievirus is a virus that belongs to the Picornaviridae family. These viruses are divided into group A and group B. In general, group A coxsackieviruses infect the skin and mucous membranes, causing febrile pharyngitis, hand, foot, and mouth disease, herpangina, and conjunctivitis. This virus is also one of the most common causes of aseptic meningitis that usually occurs in the late summer months. Group B coxsackieviruses tend to infect the heart and the pleura, as well as the pancreas. Infection of the heart can lead to myocarditis, and dilated cardiomyopathy and can lead to pericardial effusions. Recently, the development of type 1 diabetes mellitus has been associated with previous coxsackievirus B infection.
Play Video + QuizView Rubella (German Measles)

Rubella is a viral exanthem that occurs in both children and adults. It is caused by the rubella virus, which is an enveloped, single-stranded icosahedral RNA virus, and is a member of the togavirus family. It is also known as the German measles or the three-day measles. Rubella can present with fever and tender postauricular lymphadenopathy. Following this is a diffuse, light pink maculopapular rash that first appears on the face and then spreads to the trunk and extremities within 24 hours. The rash usually lasts about three days, hence the name three-day measles. Adults can also have arthritis. In pregnancy, rubella is a TORCH infection and can cause serious complications, including hearing loss, ocular and cardiovascular defects, and mental retardation.
Play Video + QuizFifth’s Disease

Erythema infectiosum or Fifth’s Disease is a mild viral infection that is characterized by the slapped face appearance. It typically occurs in school-age children; however, adults can contract the disease. Pain and swelling in the joints (polyarthropathy syndrome) is a common finding in adult women with the disease. It is transmitted by respiratory secretions, blood, and blood products. The period of communicability is uncertain and the incubation period is 4 to 14 days and may be as long as 21 days. Isolation is not necessary.
Play Video + QuizQuestion 1 |
Rubella Hint: Usually presents with fever, lymphadenopathy and fine maculopapular rash. | |
Roseola | |
Rubeola Hint: Typically presents with maculopapular rash with fever, conjunctivitis, cough, coryza. | |
Varicella Hint: Presents with pruritic rash that starts as erythematous maculopapular rash that become vesicles. |
Question 2 |
Rubella (German measles) | |
Varicella Hint: Presents with pruritic rash that starts as erythematous macules that become vesicles and later pustules. | |
Infectious mononucleosis Hint: Presents as fever, pharyngitis, and lymphadenopathy. | |
Rubeola (measles) Hint: Presents as maculopapular rash with fever, conjunctivitis, cough, coryza. |
Question 3 |
Measles | |
Congenital syphilis | |
Erythema infectiosum | |
Meningococcemia | |
Rubeola |
Question 4 |
Parvovirus | |
Adenovirus | |
Rhinovirus | |
Paramyxovirus | |
Herpes virus |
Question 5 |
Maternal rubella infection | |
Maternal varicella infection | |
Congenital hypothyroidism | |
Acromegaly | |
Fetal hydrops |
Question 6 |
Allergies to eggs or neomycin are not contraindications to the measles vaccine | |
Those who received killed virus immunization between 1963 and 1967 should receive a live attenuated booster vaccination | |
Infants receiving vaccination before 15 months of age do not need booster vaccinations | |
The present immunization is a genetically derived recombinant vaccine | |
Those born before 1956 should receive a measles booster vaccination |
Question 7 |
Coxsackievirus | |
Adenovirus | |
Syphilis | |
Varicella | |
Measles |
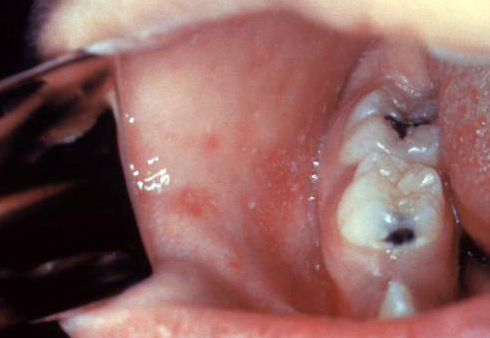
- Coxsackievirus A
- A16 is responsible for hand, foot, and mouth disease, which is characterized by stomatitis and a vesicular rash that affects the hands and feet. It is usually mild, affects young children, and may occur in epidemics.
- A2, A4, A5, A6, A7, and A10 are responsible for herpangina, which is a more severe febrile illness that sometimes leads to febrile seizures. Other symptoms include a severe sore throat; vesiculoulcerative lesions that affect the tonsils, soft palate, and posterior pharynx; headaches; myalgias; and vomiting.
- Coxsackievirus B
- B1, B2, B3, B4, and B5 are responsible for pleurodynia with pain associated with the area of diaphragmatic attachment. Other symptoms include fever, headache, sore throat, malaise, and vomiting. Orchitis and pleurisy may also occur.
|
List |