Patient will present as → a 35-year-old male presents to the clinic with a painful, swollen finger that started three days ago. He reports a history of a puncture wound to the pad of his right index finger while working with wood. Since then, he has noticed increasing redness, swelling, and throbbing pain that worsens when the finger is elevated. He denies fever or systemic symptoms. On physical examination, the distal pulp of the right index finger is erythematous, tense, and warm to the touch. There is tenderness to palpation, with fluctuance, suggesting a localized abscess. The range of motion of the finger is limited due to pain. The patient is diagnosed with a felon, likely caused by Staphylococcus aureus introduced via the puncture wound. Management includes incision and drainage (I&D) to evacuate the abscess and relieve pressure in the finger pulp. A longitudinal incision is made over the affected area to prevent damage to neurovascular structures, and the wound is irrigated thoroughly. A culture is obtained to guide antibiotic therapy. Empiric treatment with an oral antibiotic effective against methicillin-resistant Staphylococcus aureus (MRSA), such as clindamycin or trimethoprim-sulfamethoxazole, is initiated. The patient is instructed to keep the finger elevated, perform warm soaks several times a day, and follow up in 48 hours to monitor for improvement. Signs of worsening infection, such as fever, increasing pain, or spreading erythema, are discussed with the patient, requiring urgent reevaluation.
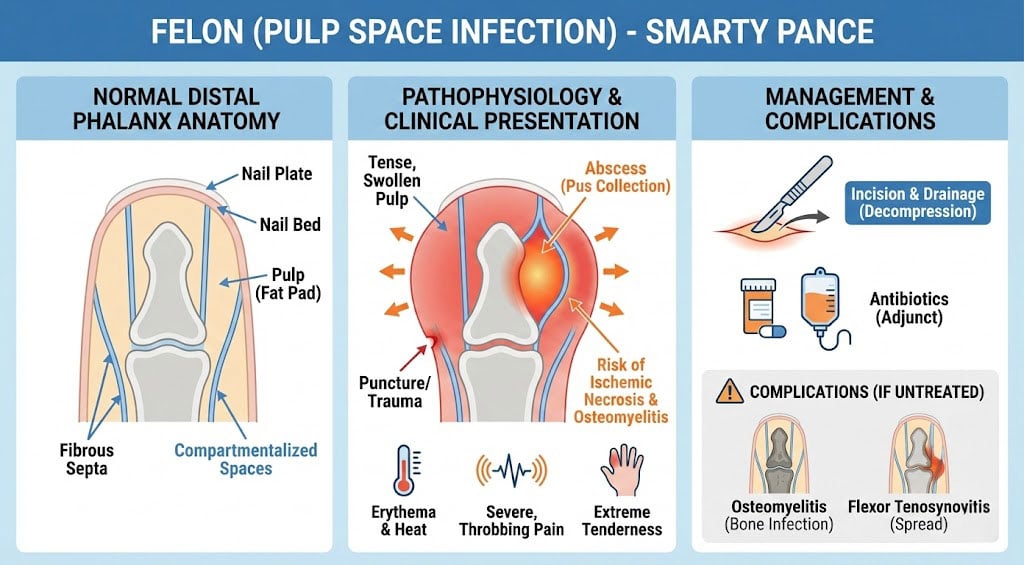
Felon is an infection of the fingertip pulp space, usually involving the thumb and index finger, typically caused by bacterial invasion, leading to a closed-space abscess
- Penetrating trauma (e.g., splinters, nail biting) is the most common cause, but it can also be a complication of untreated раrοոyсhia
- The most common site is the distal pulp, which may be involved centrally, laterally, or apically
- Most cases are caused by Staphylococcus aureus, including MRSA
- Symptoms include severe throbbing pain, swelling, warmth, and erythema localized to the distal fingertip; may also exhibit tense pressure and fluctuation if an abscess has formed
.jpg)
Apical felon
Diagnosis is clinical, based on characteristic symptoms and physical findings
- Imaging (e.g., X-ray) may be needed to rule out osteomyelitis or foreign bodies
- Ultrasound can confirm the presence of an abscess
Early cases can be managed with warm soaks, elevation, and oral antibiotics (e.g., cephalexin for MSSA or clindamycin/TMP-SMX for MRSA coverage)
- Abscess formation requires incision and drainage (I&D) performed with either a longitudinal or lateral approach, avoiding transverse incisions to prevent neurovascular damage or damage to the flexor tendon sheath
- Culture is obtained to guide antibiotic therapy, and antibiotics should follow I&D if signs of systemic infection or cellulitis are present
- Complications include osteomyelitis, tendon sheath infection, or septicemia if left untreated
Question 1 |
Streptococcus pyogenes Hint: While Streptococcus pyogenes is a common cause of skin infections, such as cellulitis and erysipelas, it is less commonly associated with felons than Staphylococcus aureus. | |
Staphylococcus aureus | |
Eikenella corrodens Hint: Eikenella corrodens is typically associated with human bite wounds and is not a common pathogen in felons caused by minor trauma. | |
Pseudomonas aeruginosa Hint: Pseudomonas aeruginosa can cause skin infections, particularly in individuals with compromised immune systems or those exposed to contaminated water, but it is not the most common cause of felons. | |
Pasteurella multocida Hint: Pasteurella multocida is associated with animal bite wounds, particularly cat bites, and is not typically implicated in felons resulting from minor trauma in a healthy individual. |
Question 2 |
Decreased capillary refill in the affected digit Hint: Decreased capillary refill may be present but is a nonspecific finding that can occur in many digital conditions. | |
Pain on passive extension of the digit Hint: Pain on passive extension is more characteristic of flexor tenosynovitis and follows Kanavel's signs. | |
Fluctuance of the volar pad | |
Drainage from the nail fold Hint: Drainage from the nail fold is characteristic of paronychia, not a felon. | |
Pain on lateral compression of the digit Hint: Pain on lateral compression is more commonly associated with paronychia or early cellulitis. |
Question 3 |
Oral antibiotics alone Hint: al antibiotics alone are insufficient once an abscess has formed and fluctuance is present. Surgical drainage is necessary. | |
Warm compresses and elevation Hint: Warm compresses and elevation may help early in the course but are inadequate once fluctuance has developed. | |
Needle aspiration of the abscess Hint: Needle aspiration is generally inadequate due to the multiple septated compartments within the pulp space. | |
Longitudinal volar incision and drainage | |
Conservative management with observation Hint: Conservative management with observation is inappropriate when fluctuance is present, as this can lead to tissue necrosis and complications. |
|
List |
References: Merck Manual · UpToDate