 Lecture
Lecture


A 15-year-old male with knee pain
Patient will present as → a 13-year-old male who comes to the clinic with his parents, complaining of progressive pain just below his right knee that worsens with activity, especially after soccer practice. The pain has been intermittent over the past few months but has recently become more consistent. He denies any trauma or injury. His medical history is unremarkable. On physical examination, there is notable swelling and tenderness over the tibial tuberosity of the right knee. The pain is exacerbated by knee extension against resistance. Radiographs of the knee show no fractures but reveal swelling over the tibial tuberosity with some lifting of the tubercle apophysis consistent with Osgood-Schlatter disease. The patient is advised to limit activities that exacerbate symptoms, apply ice after activity, and consider physical therapy for stretching and strengthening exercises. An over-the-counter pain reliever is recommended for symptom management.

To watch this and all of Joe Gilboy PA-C's video lessons you must be a member. Members can log in here or join now.
Osgood–Schlatter Disease is an overuse traction apophysitis of the tibial tubercle caused by repetitive pulling of the patellar tendon during periods of rapid growth.
- It most commonly occurs in adolescents (boys aged 12-15; girls aged 11-12) who are undergoing a rapid growth spurt
- The primary risk factor is participation in sports that involve running, cutting, and jumping, as these activities place excessive stress on the tibial tubercle through repetitive contraction of the quadriceps muscle
- Repetitive traction of the apophysis of the tibial tuberosity results in microtrauma and micro-avulsion - the proximal patellar tendon insertion separates from the tibial tubercle
- Localized tenderness and swelling over the tibial tuberosity
- Pain on resisted knee extension with a lump below the knee and a prominent tibial tuberosity
- Pain is activity-related and improves with rest
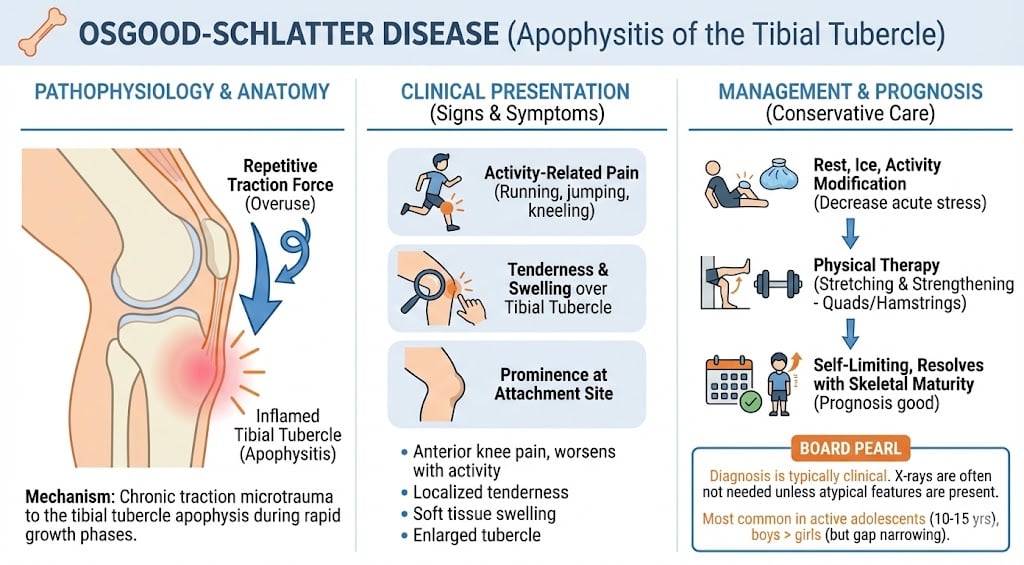
Osgood-Schlatter disease is a clinical diagnosis based on history. Additional signs and symptoms include anterior knee pain that increases over time, an enlarged tibial tubercle, and localized edema
- Diagnostic imaging with a lateral radiograph of the knee
- For atypical presentation (pain not related to activity, fever, rash, etc.) to exclude other conditions (e.g., osteomyelitis)
- Soft tissue swelling and loss of sharp margins of the patellar tendon in the acute phase, and bone fragmentation at the tibial tuberosity in the late phase

Lateral radiograph in Osgood Schlatter disease - note the fragmentation and irregularity of the tibial tubercle
Benign and self-limiting
- Conservative analgesics, ice, and physical therapy - first-line treatment for Osgood-Schlatter disease
- Operative - ossicle resection and/or excision of the tibial tuberosity - considered in patients who do not respond to conservative management and after skeletal maturity
 Osmosis Osmosis |
|
 |

Osgood-Schlatter disease involves apophysitis of the proximal tibial tubercle often due to overuse. Active, young boys who have experienced a recent growth spurt and partake in running and jumping activities are most at risk for this condition. Osgood-Schlatter disease is a clinical diagnosis based on history; additional signs and symptoms include anterior knee pain that increases over time, an enlarged tibial tubercle, and localized edema. Since this condition is often self-limiting, treatment is conservative and consists of rest, activity restriction, and NSAIDs.
Play Video + QuizQuestion 1 |
Family history of gout Hint: Gout is an inflammatory arthritis due to uric acid crystal deposition, unrelated to Osgood-Schlatter. | |
High body mass index (BMI) Hint: While being overweight can put extra stress on joints, it's not a specific risk factor for Osgood-Schlatter. | |
Participation in sports requiring repetitive quadriceps loading | |
Recent viral upper respiratory infection Hint: Viral infections do not play a role in the development of Osgood-Schlatter. | |
Trauma to the anterior knee Hint: A direct injury might cause pain, but not the chronic process of Osgood-Schlatter. |
Question 2 |
Complete blood count (CBC) Hint: CBC is for general health assessment; findings are usually normal in Osgood-Schlatter. | |
Erythrocyte sedimentation rate (ESR) Hint: ESR is used for inflammation, not routinely needed for Osgood-Schlatter. | |
Knee aspiration and synovial fluid analysis Hint: Done for suspected infections or crystal arthropathies. | |
Plain radiograph (X-ray) of the knee | |
Rheumatoid factor (RF) Hint: RF is associated with rheumatoid arthritis, not Osgood-Schlatter. |
Question 3 |
Complete cessation of sports Hint: While temporary rest from exacerbating activities is needed, complete sports withdrawal can be detrimental. | |
Immediate physical therapy referral Hint: PT can be beneficial, but the first step is usually activity modification and pain control. | |
NSAIDs and activity modification | |
Prescription of custom orthotics Hint: These can be considered, but not typically the primary intervention. | |
Surgical intervention Hint: Surgery is reserved for very rare, severe cases that don't respond to conservative measures. |
|
List |
References: Merck Manual · UpToDate