You have completed family medicine EOR topics:
Family Medicine EOR Urology/Renal Topic List |
Q
Flashcards ready when you areYou have opened several Quizlet sets recently. Loading this one only when needed helps prevent a temporary Quizlet limit.
|
| Balanitis |
Patient will present as → a 33-year-old male presents with a 3-day history of redness, swelling, and soreness of the glans penis. He also reports a foul-smelling discharge and discomfort during urination. He has a history of type 2 diabetes mellitus, which is poorly controlled. On examination, the glans penis is erythematous with erosions and a whitish discharge. There is no evidence of urethral discharge or inguinal lymphadenopathy. The patient is diagnosed with balanitis, likely fungal in origin, given his diabetes status. A swab of the discharge is taken for culture to confirm the diagnosis. He is prescribed a topical antifungal cream and advised on proper genital hygiene. The importance of better glycemic control is emphasized to prevent recurrent infections. He is scheduled for a follow-up to reassess his response to treatment and to discuss his diabetes management. Inflammation of the foreskin and head of the penis
- Balanitis is most common in uncircumcised men
- Causes include skin disorders, infection, poor hygiene, uncontrolled diabetes, and harsh soaps
- Symptoms include pain, redness, and a foul-smelling discharge from under the foreskin
- Risk factors include DM, poor hygiene, and irritants
DX: Balanitis should be suspected in men who complain of penile pain and/or redness.
- If available, a potassium hydroxide (KOH) stain can be examined by microscopy for budding yeast and/or pseudohypha
TX: Depends on the cause:
- Topical antifungal agents: clotrimazole 1% or miconazole 2%, each applied twice daily for one to three weeks
- If there is no improvement with antifungals - hydrocortisone 1% cream or ointment twice daily for seven days for nonspecific dermatitis
- For suspected anaerobic infection: metronidazole 0.75% applied twice daily for seven days
- In extreme cases, the foreskin may need to be removed (circumcision)
 Balanitis on an uncircumcised penis |
| Benign prostatic hyperplasia |
Patient will present as → a 65-year-old man presents to your clinic complaining of frequent urination, especially at night, and a sensation that his bladder is not completely emptying. He also reports a weak urinary stream and occasional dribbling. He has no history of urinary tract infections, hematuria, or renal stones. His medical history is significant for hypertension, for which he takes hydrochlorothiazide. On digital rectal exam, his prostate is uniformly enlarged, firm, and rubbery. Urinalysis is unremarkable, and his serum prostate-specific antigen (PSA) level is 5. A disease of elderly men (average age is 60 to 65 years caused by hyperplasia of prostatic epithelial, stromal cells → formation of nodules in periurethral (transition) zone → narrowing of urethral canal → urethral compression → obstruction of the urinary outlet
- 50% of men develop BPH by 60 and > 90% by age 85
- Features: A decreased force of urinary stream, hesitancy (stop and start) and straining, postvoid dribbling, incomplete emptying, frequency, nocturia, urgency, recurrent UTIs
- In men with BPH, avoid the use of anticholinergic and antihistamines
- This type of prostate enlargement isn't thought to be a precursor to prostate cancer
DX: Accurately diagnosing BPH is extremely important as more serious conditions, such as prostate cancer, must be ruled out
- DRE ⇒ enlarged rubbery prostate
- Urinalysis/Culture → Microscopic hematuria may be present → Pyuria, bacteriuria in case of concomitant UTI
- Blood tests → Often PSA often elevated > 4 → Electrolytes, blood urea nitrogen (BUN), and creatinine to evaluate for renal impairment
- Ultrasound → Evaluate bladder size, prostate size, degree of hydronephrosis
- Cystoscopy → Reveal bladder diverticula/calculi before scheduled invasive treatment
TX: includes medications that relax the bladder or shrink the prostate, surgery, and minimally invasive surgery
- Conservative measures, e.g., decrease fluid intake before bedtime/going out; avoid caffeine and alcohol (mild diuretic effects)
- Alpha-adrenergic receptor blockers (terazosin, tamsulosin) → decrease prostate, bladder, and urethral muscle tone
- 5-alpha reductase inhibitors (finasteride) → decrease DHT synthesis → reduce prostate gland size
- Phosphodiesterase-5 enzyme inhibitors (e.g., tadalafil) → induce smooth muscle relaxation
- TURP (transurethral resection of the prostate) if refractory to meds → removes excess prostate tissue to relieve obstruction - sexual dysfunction and urinary incontinence
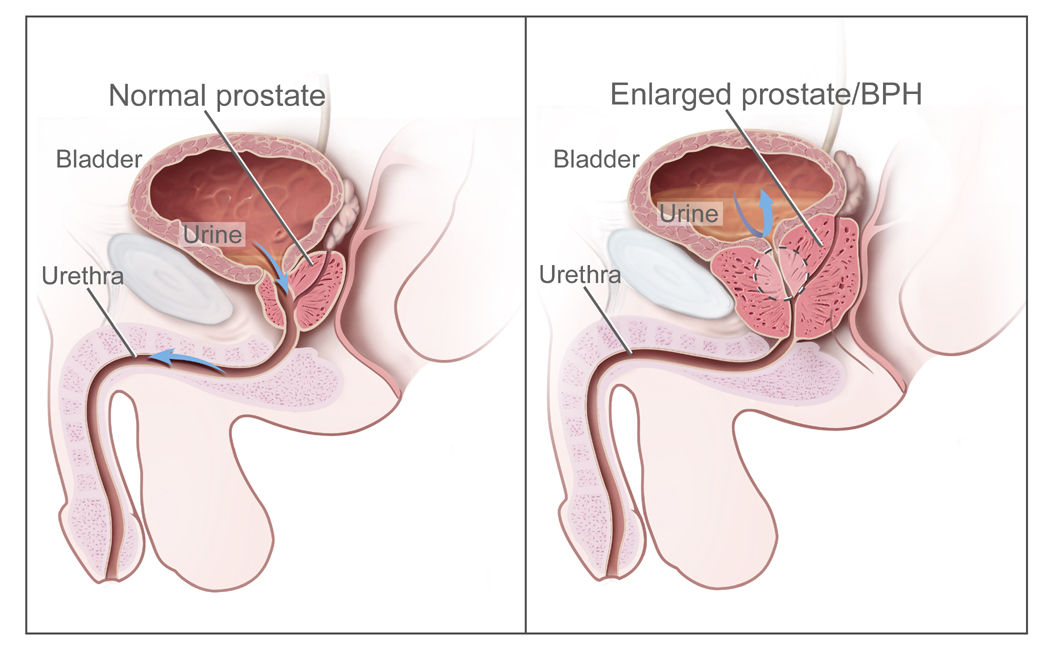 The panel on the left shows the normal prostate and the flow of urine from the bladder through the urethra. The panel on the right shows an enlarged prostate pressing on the bladder and urethra, blocking the flow of urine. |
| Chlamydia |
Patient will present as → a 21-year-old male complaining of pain on urination and a watery discharge from his penis. Gram stain of the discharge is negative for bacteria but shows many neutrophils. When questioned about his social history, he says that he uses condoms most of the time but occasionally has unprotected sex. The patient responds to treatment with azithromycin. The most common sexually transmitted infections
- Gram-negative rod. Intracellular
- Asymptomatic, dysuria
Men: typically present with nongonococcal urethritis (mucoid or watery/clear urethral discharge and dysuria). The discharge is often only seen upon milking the urethra. Also, a common cause of epididymitis in men
Women: most females with C. trachomatis infections are asymptomatic but can cause cervicitis, urethritis, and pelvic inflammatory disease in women
- Cervicitis is characterized by vaginal discharge, vaginal bleeding, cervical erythema, and friability
- Urethritis is characterized by symptoms of a urinary tract infection (UTI), such as frequency and dysuria
- Pelvic inflammatory disease characterized by lower abdominal pain, cervical discharge, and irregular vaginal bleeding
- If unnoticed or untreated in women, these infections can result in infertility, miscarriage, and an increased risk of a mislocated pregnancy
DX: Nucleic acid amplification test (NAAT) is the gold standard
- Gram stain reveals no organisms
TX: (1) Doxycycline 100 mg PO two times per day for 7 days
- Alternative regimens include azithromycin 1 g orally in a single dose OR levofloxacin 500 mg orally once daily for 7 days
- Persons who receive a diagnosis of chlamydia should be tested for HIV, Gonorrhea, and syphilis
- All individuals with a positive NAAT for N. gonorrhoeae warrant treatment for gonorrhea in addition to chlamydia, even if they are asymptomatic.
- Those who have a negative NAAT for N. gonorrhoeae do not need additional treatment for gonorrhea
- Treatment for gonorrhea ⇒ Ceftriaxone 500 mg IM x 1
- Treat partners and educate to refrain from sex until the infection is treated
- Sex partners should be referred for evaluation, testing, and presumptive treatment if they had sexual contact with the partner during the 60 days preceding the patient’s onset of symptoms or chlamydia diagnosis
- The most recent sex partner should be evaluated and treated, even if the time of the last sexual contact was >60 days before symptom onset or diagnosis.
- In pregnancy, (1) azithromycin 1 g orally in a single dose or (2) amoxicillin 500 mg orally 3 times/day for 7 days
Chlamydia and gonorrhea screening the USPSTF recommends:
For sexually active women (including pregnant persons), screen for chlamydia and gonorrhea if they are
- 24 years or younger
- 25 years or older and at increased risk for infection
For sexually active men:
- The USPSTF found that the evidence is insufficient to assess the balance of benefits and harms of screening for chlamydia and gonorrhea in men. More research is needed.
 Chlamydia trachomatis in a female |
|
Patient will present as → a 34-year-old woman with a 3-day history of hematuria, dysuria, increased urinary frequency, and nocturia. She has had no fever, chills, or back pain. On examination, she does not look ill. Her temperature is 37.5 ° C. Her abdomen is nontender. There is no CVA tenderness. Cystitis is inflammation of the bladder, typically caused by a bacterial infection leading to symptoms of pelvic pain, frequent and urgent urination, and hematuria
- Characterized by dysuria WITHOUT urethral discharge. E. coli (most common)
- Dysuria, urgency, frequency, hematuria, new-onset incontinence (in toilet-trained children). Abdominal or suprapubic pain
- Absence of fever, chills, or flank pain. Change in urine color/odor
DX: Urine dipstick: nitrite, leukocyte esterase
- Urinalysis: pyuria, bacteriuria +/− hematuria +/− nitrites
- Urine culture (gold standard)
- > 100k CFU/mL (women)
- > 1000 CFU/mL men or cath patients
- → takes 24 hours to obtain results
Treat with Nitrofurantoin (not over age 65), Bactrim, Fosfomycin
- Ciprofloxacin- reserved for complicated cases
- Postcoital UTI: single-dose TMP-SMX or cephalexin may reduce the frequency of UTI in sexually active women
Lower UTI in pregnancy
- Nitrofurantoin (Macrobid): 100 mg PO BID × 7 days
- Cephalexin (Keflex): 500 mg PO BID × 7 days
Interstitial cystitis: A chronic inflammation of the bladder wall, characterized by pelvic pain, urinary frequency, and urgency, which can severely impact quality of life
- Symptoms are relieved with voiding. Diagnosis of exclusion
- Hunner’s ulcer on cystoscopy
|
| Epididymitis |
Patient will present as → a 25-year-old male with a dull, achy scrotal pain that has been gradually increasing over the last several days. He also reports pain with urination. Physical exam reveals a swollen right testicle with substantial induration. Urinalysis reveals positive leukocyte esterase and 20 WBC/HPF. Raising the testicle makes the pain less intense. ( + Prehn’s sign = relief with elevation is a classic sign – compare this to testicular torsion) Acquired by the retrograde spread of organisms through vas deferens
- The pathogen is based on the patient's age and risk factors:
- men < 35 chlamydia and gonorrhea
- men > 35 E.coli
Epididymitis is characterized by dysuria, unilateral dull aching scrotal pain that can radiate up the ipsilateral flank
- Swollen epididymis tender; fever/chills
- + Prehn's sign = relief with elevation is a classic sign
Dx: Urinalysis reveals pyuria and bacteriuria; cultures are positive for suspected organisms
TX: Supportive care: bed rest, scrotal elevation, analgesics
- Over 35- E. coli
- Levofloxacin (Levaquin) 500 mg/day PO for 10 days (21-30 days if associated prostatitis)
- For patients who are unable to take fluoroquinolones, trimethoprim-sulfamethoxazole (one double-strength tablet twice a day for 10 days) is a good alternative
- Under 35 – Gonorrhea and chlamydia
- Doxycycline 100 mg PO BID for 10 days PLUS ceftriaxone 500 mg IM × 1 (or 1 g if the patient weighs 150 kg or greater)
- Refer sexual partner(s) for evaluation and treatment if contact within 60 days of the onset of symptoms
- Patients of any age who practice insertive anal intercourse – coverage for N. gonorrhoeae, C. trachomatis, and enteric pathogen infections
- Ceftriaxone (500 mg intramuscular injection in one dose, or 1 g if the patient weighs 150 kg or greater) PLUS a fluoroquinolone (levofloxacin 500 mg orally once daily for 10 days)
|
| Glomerulonephritis |
Acute glomerulonephritis is an inflammation of glomeruli causing protein and RBC leakage into the urine, typically caused by an immune response
Two types based on 24-hour urine protein
- Nephritic syndrome: moderate proteinuria 1-3.5 g/day
- Classic presentation: edema + HTN + hematuria + RBC Casts/dysmorphic RBCs + proteinuria 1-3.5 g/day + azotemia
- Nephrotic syndrome: severe proteinuria > 3.5 g/day
- Massive edema
- Fatty casts with “maltese cross” sign
- Hypoalbuminemia, hyperlipidemia, and lipiduria
- Oval fat bodies
Nephritic syndrome:
Patient will present as → a 26-year-old man who presents with hematuria, periorbital edema, and jaundice. He has a medical history of opioid use disorder with prior hospitalizations for a heroin overdose. He is on methadone but is non-adherent. His blood pressure is 155/102 mmHg. Physical examination is significant for scleral icterus, hepatomegaly, and palpable purpura. Serology shows decreased C3 and C4 levels and elevated anti-hepatitis C antibodies. Urinalysis demonstrates dysmorphic red blood cells and red blood cell casts.
- Manifestations: proteinuria, HTN, azotemia, oliguria (<400 ml urine/day), hematuria (RBC casts) hallmark, edema is not as much as nephrotic syndrome
- Urinalysis: proteinuria < 3.5 grams per day, hematuria, RBC casts
- Biopsy: hypercellular, immune complex deposition
Several etiologies of acute glomerulonephritis
- IgA Nephropathy (Berger disease) - most common cause of acute glomerulonephritis worldwide - often affects young males within days (24-48 hours) after URI or GI infection - caused by IgA immune complexes which are the first line of defense in respiratory and GI secretions so infections cause an overproduction which then damages the kidneys. Diagnosed by (+) IgA deposits in mesangium and with immunostaining
- Postinfectious - Group A strep - 10-14 days after infection - diagnosed with ASO titers and low serum complement - treatment is supportive + antibiotics
- Membranoproliferative glomerulonephritis - due to SLE, viral hepatitis
- Rapidly progressive glomerulonephritis - crescent formation on biopsy due to fibrin and plasma protein deposition
- Goodpasture's syndrome: (+) anti-GBM antibodies, dx linear IgG deposits, treat with high dose steroids, plasmapheresis + cyclophosphamide
- Vasculitis - lack of immune deposits (+) ANCA antibodies
- Microscopic polyangiitis (+) P-ANCA
- Granulomatosis with polyangiitis (Wegener's) (+) C-ANCA
Nephrotic Syndrome:
Patient will present as → a 6-year-old boy who is brought to the emergency department by his mother due to swelling around his eyes and legs. The mother reports that the patient recently recovered from an upper respiratory tract infection. Physical exam is significant for periorbital and lower extremity edema. Laboratory testing is significant for hypoalbuminemia and normal complement levels. Urinalysis demonstrates 4+ protein and fatty casts with a “maltese cross” sign. Nephrotic syndrome is defined as urinary excretion of > 3 g of protein in a 24-hour urine sample due to a glomerular disorder plus edema and hypoalbuminemia
The most common primary causes are:
- Membranous nephropathy: most common in non-diabetic adults associated with malignancies.
- Caused by immune complex formation in the glomerulus - basement membrane becomes damaged
- Minimal change disease: most common cause in kids. Assume minimal change disease if a child with idiopathic nephrotic syndrome improves after treatment with corticosteroids.
- The cause and pathogenesis of minimal change disease is unclear and it is currently considered idiopathic.
- Focal segmental glomerulosclerosis (FSGS): obese patients, heroin, and HIV+ black males.
- Primary, when no underlying cause is found
- Secondary, when an underlying cause is identified
- Toxins and drugs such as heroin and pamidronate
- Familial forms
- Secondary to nephron loss and hyperfiltration, such as with chronic pyelonephritis and reflux, morbid obesity, diabetes mellitus
The most common secondary causes are:
- Lupus: both nephritic and nephrotic
- Diabetes: a common cause of nephrotic syndrome and subsequent renal failure
- Preeclampsia
|
| Gonorrhea |
Patient will present as → a 19-year-old sexually active woman presents to your office with complaints of yellow vaginal discharge and intermittent postcoital vaginal bleeding for 1 week. She otherwise feels well. On examination, there is purulent discharge visible in the endocervical canal. After you collect vaginal fluid for a wet prep and cervical samples for gonorrhea and chlamydia cultures, you note bleeding at the cervical os. On bimanual examination, the patient complains of tenderness on cervical palpation but denies uterine or adnexal tenderness. Wet prep reveals vaginal pH 4; negative whiff; 20 white blood cells (WBCs) per high-power field; and no clue cells, trichomonads, or pseudohyphae. Caused by Neisseria gonorrhoeae - a gram-negative diplococcus
Presentation:
- Women: often asymptomatic. Prolonged infection can result in pelvic inflammatory disease when the bacterium travels into the pelvic peritoneum.
- Men: yellow, creamy, profuse, and purulent discharge
DX: Diagnose with ligase chain reaction assay of discharge or urine
TX: High dose IM ceftriaxone
- For individuals who weigh < 330 lbs – ceftriaxone 500 mg intramuscular (IM) in a single dose
- For individuals who weigh ≥ 330 lbs – ceftriaxone 1 g IM in a single dose
- When ceftriaxone cannot be used because of cephalosporin allergy, a single 240 mg IM dose of gentamicin plus a single 2 g oral dose of azithromycin is an option
- Treat partners and educate them to refrain from sex until the infection is treated
- Treatment for coinfection with Chlamydia trachomatis with oral doxycycline (100 mg twice daily for 7 days) should be administered when a chlamydial infection has not been excluded
Gonococcal pharyngitis is usually asymptomatic but may cause a sore throat
- Neonatal conjunctivitis and pharyngitis
- Disseminated infections can occur, resulting in septic arthritis, tenosynovitis, and pustules on the hands and feet. Commonly affects the knee joint
Chlamydia and gonorrhea screening the USPSTF recommends:
For sexually active women (including pregnant persons), screen for chlamydia and gonorrhea if they are
- 24 years or younger
- 25 years or older and at increased risk for infection
For sexually active men:
- The USPSTF found that the evidence is insufficient to assess the balance of benefits and harms of screening for chlamydia and gonorrhea in men. More research is needed.
 Gonorrhea infection in male penis showing thick, yellow, creamy, and purulent discharge |
| Hernias |
A hernia is a protrusion of an organ or structure through the wall that normally contains it. The type of hernia is indicated by its location.
Inguinal hernias:
- Indirect Inguinal Hernia (Most Common): Passage of intestine through the internal inguinal ring down the inguinal canal, may pass into the scrotum. Often congenital and will present before age one.
- Remember: Indirect goes through the Internal Inguinal Ring (an “I” for an “I”)
Patient will present as → a 20-year-old male presents with a swelling in his right groin that has been increasing in size over the past six months. He notes that the bulge is more noticeable when standing and disappears when lying down. It is not painful but causes discomfort during physical activities. On examination, a soft mass is palpable in the right inguinal canal and extends into the scrotum, indicative of an indirect inguinal hernia. He is referred to a general surgeon for elective surgical repair to prevent potential complications.  Indirect inguinal hernia on right side
- Direct Inguinal Hernia: Passage of intestine through the external inguinal ring at Hesselbach's triangle, rarely enters the scrotum
Patient will present as → a 60-year-old male with a history of chronic cough due to COPD presents with a bulge in his right groin area. He reports that the bulge has been present for a year and is becoming more uncomfortable. On examination, there is a reducible mass in the right inguinal region, medially located to the inferior epigastric vessels, consistent with a direct inguinal hernia. Due to his symptoms and the risk of complications, he is referred to a general surgeon for consideration of surgical repair.  Direct inguinal hernia on the right Hernias of various types can entrap the intestines and cause an intestinal blockage – this is called an “ incarcerated hernia” and is a medical emergency
- Obstructed hernia: This is an irreducible hernia containing intestine that is obstructed from without or within, but there is no interference to the blood supply to the bowel.
- Incarcerated hernia: A hernia so occluded that it cannot be returned by manipulation. It may or may not become strangulated. Incarcerated hernias are often surgical emergencies, and a surgeon should be consulted early.
- Strangulated hernia: A hernia becomes strangulated when the blood supply of its contents is seriously impaired
|
| Nephrolithiasis |
Patient will present as → a 31-year-old man with right flank pain radiating into the scrotum, gross hematuria, right-sided hydronephrosis, and normal abdominal x-ray Urinary calculi are solid particles in the urinary system
- They may cause colicky flank pain radiating to the groin, hematuria, CVA tenderness (also a symptom of pyelonephritis), nausea and vomiting, and chills/fever due to secondary infection
Four types:
- Calcium oxalate (80%): Most common, excess oxalate, hyperparathyroidism, radiopaque - avoid grapefruit juice (makes calcium oxalate stones worse)
- Struvite (10%): Associated with chronic UTI with Klebsiella and Proteus species, radiopaque
- Uric Acid (7%): Form in individuals with persistently acidic urine - Excess meat/alcohol, gout, radiolucent
- Cystine (1%): Rare genetic, radiolucent (young boy with kidney stones)
DX: CT scan (spiral CT) without contrast of the abdomen and pelvis is the gold standard for diagnosis
- Urinalysis will often show microscopic hematuria
- Cannot determine the type of stone from CT so give the patient a strainer and have them strain the urine so you can catch the stone as it passes for identification
- Serum chemistry—obtain BUN and Cr levels (for evaluation of renal function) and also calcium, uric acid, and phosphate levels
TX:
General measures (for all types of stones)
- Analgesia: IV morphine, parenteral NSAIDs (ketorolac)
- Vigorous fluid hydration—beneficial in all forms of nephrolithiasis
- Antibiotics—if UTI is present
- Alpha-blocker therapy (Flomax) for patients with symptomatic ureteral stones >5 mm and ≤10 mm to facilitate ureteral stone passage (usually given to most patients independent of size)
- Outpatient management is appropriate for most patients. Indications for hospital admission include:
- Pain not controlled with oral medications
- Anuria (usually in patients with one kidney)
- Renal colic plus UTI and/or fever
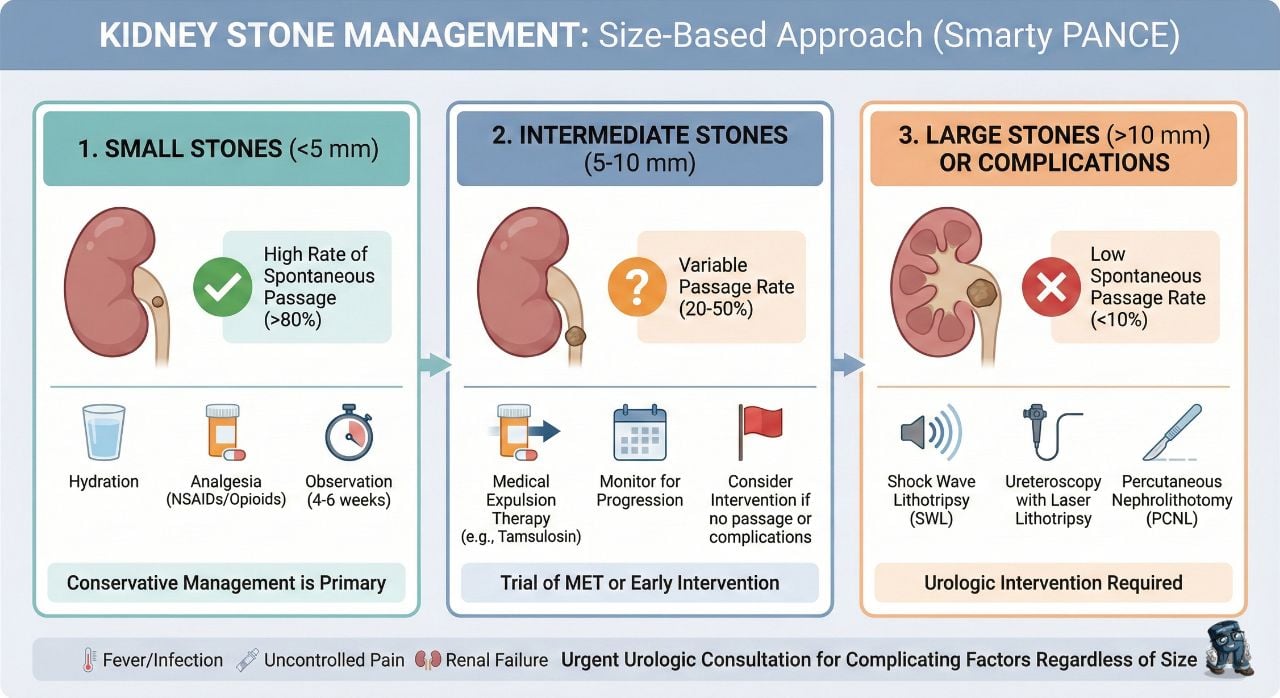
Stones < 5 mm will have an 80% chance of spontaneous passage
- Stones > 5 – 10 mm have a 20% chance of passage and may require elective lithotripsy – patients should be considered for early elective intervention
- Stones > 10 mm are not likely to pass spontaneously. Ureteral stent or percutaneous nephrostomy (gold standard) should be used if renal function is jeopardized. Urgent treatment with extracorporeal shock wave lithotripsy can be used for renal stones of less than 2 cm or for ureteral stones of less than 10 mm
|
| Orchitis |
Patient will present as → a 31-year-old male complaining of unilateral scrotal swelling with pain radiating to the ipsilateral groin. Examination reveals a tender, swollen testicle, scrotal edema with erythema, and shininess of the overlying skin. Orchitis is an inflammation of the testicles. It can be caused by either bacteria or a virus
- Commonly caused by ascending bacterial infection from the urinary tract
- Occurs in 25% of postpubertal males with MUMPS
- Unilateral swollen testicle/tenderness with erythema and shininess of the overlying skin, fever/tachycardia
- Orchitis is rarely seen without epididymitis unless the patient has mumps
DX: UA reveals pyuria and bacteriuria with a bacterial infection
TX: If mumps is the cause, treat mumps (+ ice/analgesia)
If bacteria is the cause, treat it like epididymitis
- Age <35 or sexually active postpubertal males (cover for GC/Chlamydia)
- Ceftriaxone 500 mg IM once PLUS doxycycline 100 mg PO BID for 10 days
- Azithromycin 2 g PO once PLUS doxycycline 100 mg BID if severe PCN allergy
- Age >35 (STI not suspected) - Levofloxacin 500 mg/d PO once daily for 10 days (21 days if associated prostatitis)
|
| Prostatitis |
Patient will present as → a 63-year-old man with a history of benign prostatic hyperplasia who reports 3 days of fever, chills, and pain with urination. He was recently catheterized during admission to the hospital. Physical exam reveals a tender and enlarged prostate on digital rectal exam. Urinalysis reveals pyuria and hematuria. Ascending infection of gram-negative rods into prostatic ducts
- Acute: sudden onset of fever, chills, and low back pain combined with urinary frequency, urgency, and dysuria
- Chronic: variable – asymptomatic ⇒ acute symptomatology
- All forms present with irritative bladder symptoms (frequency, urgency, dysuria) and some obstruction
- Physical exam reveals a tender and enlarged prostate on digital rectal exam
DX: Urinalysis will reveal pyuria and hematuria
- Prostatic fluid = leukocytosis, culture typically positive for E.coli in acute infections
- chronic usually have enterococcus
- If you suspect acute prostatitis, DO NOT massage the prostate. This can lead to sepsis!
TX:
- Men < 35: Chlamydia and Gonorrhea - ceftriaxone and doxycycline
- E coli and pseudomonas in men > 35 - treat with fluoroquinolones or Bactrim for 4-6 weeks to ensure eradication of the infection – culture urine 1 week after the conclusion of therapy
- Hospitalization in acute - may need parenteral fluoroquinolones
- If the fever doesn’t resolve in 36 hours, suspect abscess and consult urology
- Chronic prostatitis is treated with fluoroquinolones or Bactrim x 6-12 weeks
- NSAIDs = effective for analgesia; alpha 1 blocker may be helpful if lower UTI symptoms are present
- Chronic, recurrent, resistant prostatitis with/without prostatic calculi may require transurethral resection of the prostate (TURP) for resolution
|
| Pyelonephritis |
Patient will present as → a 32-year-old female presents with fever, chills, nausea, and flank pain for 24 hours. She developed dysuria and urinary frequency 3 days prior and states that both have worsened. On physical exam, you note suprapubic abdominal pain and CVA tenderness. The urinalysis reveals white blood cell casts. Irritative voiding + fever + flank Pain + nausea and vomiting + CVA tenderness
DX: Urinalysis
- Pyuria, hematuria, bacteriuria, and WBC casts (pathognomonic pyelonephritis)
- Leukocyte esterase, nitrites, hematuria
- Culture and sensitivity needs to be done
- If complicated pyelonephritis order a renal ultrasound may show hydronephrosis secondary to obstruction
TX:
An oral regimen is considered the best initial outpatient treatment (7 days of outpatient treatment is equivalent to longer treatment regimens)
- Ciprofloxacin: 500 mg BID for 7 days
- Ciprofloxacin XR: 1,000 mg/day for 7 days
- Levofloxacin: 750 mg/day for 5 days
- Cephalexin 500 mg PO QID for 10-14 days
IV antibiotics are indicated for inpatients who are toxic or unable to tolerate oral antibiotics
- Ceftriaxone 1 g IV once daily
Management of acute pyelonephritis in pregnant women includes hospital admission for parenteral antibiotics.
- Empiric therapy includes IV/IM ceftriaxone
"The decision to hospitalize a patient is usually clear in the setting of critical illness or sepsis. Otherwise, general indications for inpatient management include persistently high fever (eg, >101°F/>38.4°C) or pain, marked debility, inability to maintain oral hydration or take oral medications, suspected urinary tract obstruction, and concerns regarding adherence to therapy."
|
| Testicular cancer |
Patient will present as → a 32-year-old male presents with a painless, firm mass in his right testicle that he discovered 2 weeks ago. Serum tumor markers, including alpha-fetoprotein (AFP), beta-human chorionic gonadotropin (β-hCG), and lactate dehydrogenase (LDH) are elevated. Ultrasonography confirms the presence of a testicular mass. Orchiectomy reveals a mixed germ cell tumor. A 22-year-old male who develops a firm, painless, non-tender testicular mass with elevated serum β-HCG
- Most common solid tumor in young men ages 15-40 (average age 32 years old)
- Presents as a firm, painless, non-tender testicular mass, and a feeling of heaviness in the scrotum
- The most common type of testis cancer is a germ cell tumor
- There are two main types of germ cell tumors: seminoma and non-seminomatous germ cell tumors (NSGCT)
- Risk factors include a history of cryptorchidism
DX: Diagnostic studies include ultrasound. Tumor markers: AFP, β-HCG, and LDH
TX: Treatments include surgery, radiation, and chemotherapy
 Left testicular seminoma, hypoechoic nodule, ultrasound image |
| Urethritis |
Patient will present as → a 22-year-old heterosexual male who recently started having unprotected intercourse with his new girlfriend. He now reports a painful itching and burning sensation with urination and discomfort in the urethra. He says that sometimes in the morning it appears that the walls of the meatus are stuck together with evidence of dried secretions. On exam, there is no purulent discharge. The meatus does appear red. His girlfriend does not have any symptoms. Urethritis is an infection of the urethra with bacteria (or with protozoa, viruses, or fungi) and occurs when organisms that gain access to it acutely or chronically colonize the numerous periurethral glands in the bulbous and pendulous portions of the male urethra and in the entire female urethra
- Symptoms include painful, burning, or frequent urination, or a discharge from the urethra
DX
First-void or first-catch urine and sometimes urine culture
-
- Positive leukocyte esterase on urine dipstick or having ≥ 10 WBC/HPF on microscopy is suggestive of urethritis
- Gram stain is sensitive and specific for gonorrhea in men with urethral discharge; gram-negative intracellular diplococci typically are seen
- Diagnosis by culture is not always necessary. If done, diagnosis by culture requires demonstration of significant bacteriuria in properly collected urine
- Nucleic acid amplification test allows for the specific identification of N. gonorrhoeae, C. trachomatis, M genitalium
TX:
- The preferred regimen for gonococcal infections is a single intramuscular dose of ceftriaxone (500 mg for individuals <150 kg or 1 g for individuals ≥150 kg)
- If testing results for C. trachomatis are not available at the time of treatment, presumptive therapy for chlamydia coinfection is also indicated. In such cases, doxycycline 100 mg twice daily for seven days
- Consider replacing doxycycline with azithromycin 1 g PO if compliance in question or pregnancy
|








{kind=link}
{kind=link}