 Lecture
Lecture
Patient will present as → a 15-year-old boy with severe lower abdominal pain that awoke him from sleep about 3 hours ago. The pain is sharp and radiates to the right thigh. While in the emergency room, the patient experiences one episode of vomiting. He denies any fever, dysuria, or chills. The mom reports a childhood history of cryptorchidism. Physical examination reveals normal vitals with a blood pressure of 100/60 and a temperature of 98.6F. Abdominal examination is relatively benign. Scrotal examination reveals an elevated right testis that is diffusely tender. Lifting of the right testicle DOES NOT relieve pain, and there is a loss of the cremasteric reflex. The transillumination test is negative. Doppler ultrasound shows absent blood flow in the right testis, consistent with testicular torsion. Management includes emergency surgical detorsion and bilateral orchiopexy to prevent recurrence. The patient’s prognosis depends on prompt surgical intervention, ideally within 6 hours of symptom onset.
{kind=link}

To watch this and all of Joe Gilboy PA-C's video lessons you must be a member. Members can log in here or join now.
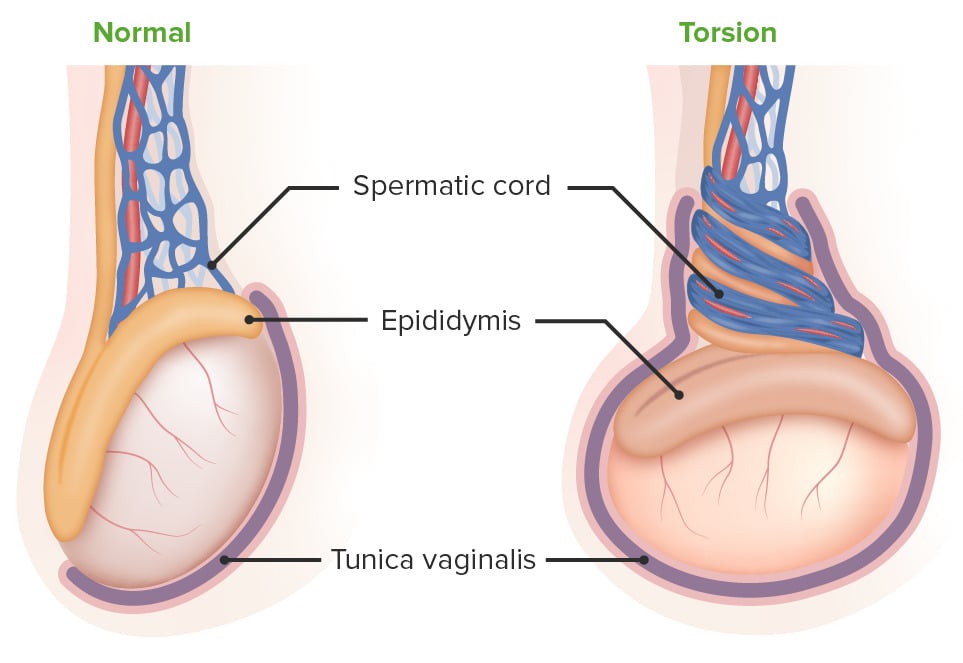
Twisting of the spermatic cord that results in compromised blood flow and ischemia - this is considered a surgical emergency
- Often triggered by vigorous physical activity, minor trauma, or during sleep
- Presents with sudden, severe unilateral scrotal pain, often accompanied by nausea and vomiting
- Most common in postpubertal adolescent males, with 65% of cases occurring between ages 10–20, though it can occur at any age
- Asymmetric high-riding testicle “bell clapper deformity”
- Negative (-) Prehn's sign (lifting of the testicle will NOT relieve pain in testicular torsion)
- Compare this to the (+) Prehn's sign = relief with elevation of the testicle, which is a classic sign of epididymitis
- Loss of cremasteric reflex (elevation of the testes in response to stroking of the inner thigh)

"The cremasteric reflex is elicited by stroking or pinching the medial thigh, causing contraction of the cremaster muscle, which elevates the testis. The cremasteric reflex is considered positive if the testicle moves at least 0.5 cm"
- Blue dot sign: Tender nodule 2 to 3 mm in diameter on the upper pole of the testicle - is indicative of the torsion of a testicular appendage, which is a vestigial remnant present in 80% of people designated male at birth
- More common in patients with a history of cryptorchidism
Diagnosis is clinical—do not delay surgical exploration if suspicion is high
- Testicular Doppler for diagnosis = best initial test
- Radionuclide scan demonstrates decreased uptake in the affected testes = gold standard
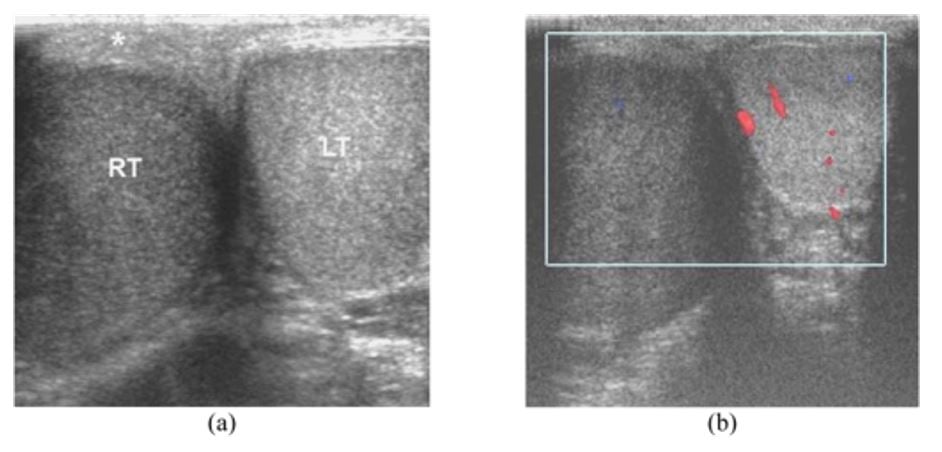
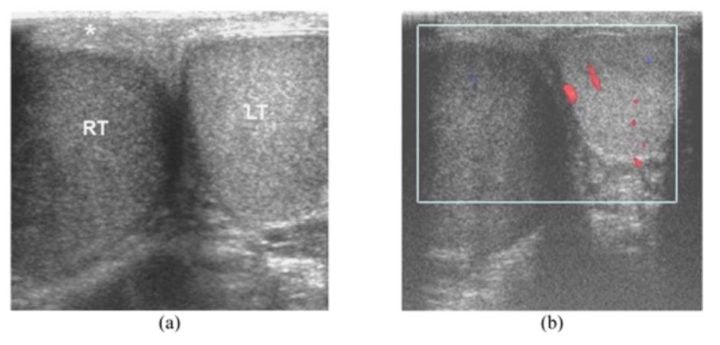
Acute testicular torsion in a 23-year-old man who presented with sudden right scrotal pain for 1 hour:a: Transverse ultrasound shows enlarged, hypoechoic right testis (RT) with thickened scrotal skin (asterisk). b: Color Doppler ultrasound shows no vascularity in the right testis. Image: 'Acute testicular torsion' by Thinyu S, Muttarak M. License: CC BY 2.5
Urgent surgical detorsion and bilateral orchiopexy must be performed within 6 hours to maximize testicular salvage
- Manual detorsion (opening a book motion) can be attempted if immediate surgery is not available, but definitive surgical fixation is still required
- Delayed treatment (>6–8 hours) significantly increases the risk of testicular infarction and loss. Salvage rates drop dramatically beyond 12 hours
- The contralateral testicle is typically fixed prophylactically to prevent recurrence

"Orchiopexy is a surgical procedure that involves permanently fixing the testicle to the scrotal wall to prevent torsion. In the setting of testicular torsion, it is performed urgently after confirming the testicle is viable during surgical exploration, and the contralateral testicle is also fixed prophylactically. The most common overall indication for orchiopexy is cryptorchidism (undescended testicle), typically performed between 6–18 months of age to reduce the risks of infertility, malignancy, and torsion."

Testicular torsion occurs when the spermatic cord twists, cutting off the testicle’s blood supply, leading to ischemia. The principal symptom is a rapid onset of testicular pain. The most common underlying cause in adolescents and neonates is a congenital malformation known as a “bell-clapper deformity” wherein the testis is inadequately affixed to the scrotum allowing it to move freely on its axis and susceptible to induced twisting of the cord and its vessels. Testicular malignancy is the most common etiology in adults. Diagnosis is clinical, with surgical detorsion urgently performed to prevent necrosis of the testicle and possible subfertility.
Play Video + QuizQuestion 1 |
Elevation of the scrotum and ice therapy | |
Ultrasound evaluation with Doppler color flow | |
Continued observation | |
Computed tomography (CT) scan of the pelvis | |
Doppler stethoscope evaluation |
Question 2 |
True | |
False |
Question 3 |
oral doxycycline Hint: Oral doxycycline is the treatment of choice for epididymitis. While epididymitis and testicular torsion present similarly, the Doppler ultrasound in epididymitis would show increased blood flow, not decreased. | |
emergent surgery | |
incision and drainage Hint: Incision and drainage is indicated for treatment of abscesses, not testicular torsion.Incision and drainage is indicated for treatment of abscesses, not testicular torsion. | |
scrotal elevation and ice packs Hint: Scrotal elevation and ice packs are indicated for adjunct treatment of epididymitis, not testicular torsion. |
Question 4 |
Nodular mass within the testis Hint: Testicular cancer is characterized by a painless nodular enlargement of the testis typically discovered by the patient. | |
High-lying testis | |
Transilluminated fluid mass Hint: A hydrocele is a collection of fluid within the scrotum which can be transilluminated on exam. | |
Palpation of a soft bag of worms Hint: A varicocele refers to varicose veins of the spermatic cord. It feels like a soft bag of worms in the scrotum separate from the testis. |
|
List |
References: Merck Manual · UpToDate