


A 5 y/o with a painless bulge in the left groin
Patient will present as → a 50-year-old man presents with a lump in his groin for 2 weeks. He states he was lifting an air conditioner and he felt a pop in his groin and began to notice an outpouching in his lower abdomen that has become mildly tender over the last week. Resting and lying flat appears to help, while standing and lifting aggravate it. He denies any fevers, nausea, vomiting, or changes in bowel habits. Patient denies any previous abdominal surgeries or procedures. Upon examination, you identify a soft, reducible mass in the lower abdomen, and hernia examination reveals a mass pushing against the side of your finger. You order an ultrasound of the lower abdomen and find the intestinal sac has traversed through a weakened area of the abdominal wall and through Hesselbach's Triangle.
A hernia is a protrusion of an organ or structure through the wall that normally contains it. The type of hernia is indicated by its location.
|
Location of common hernias
|
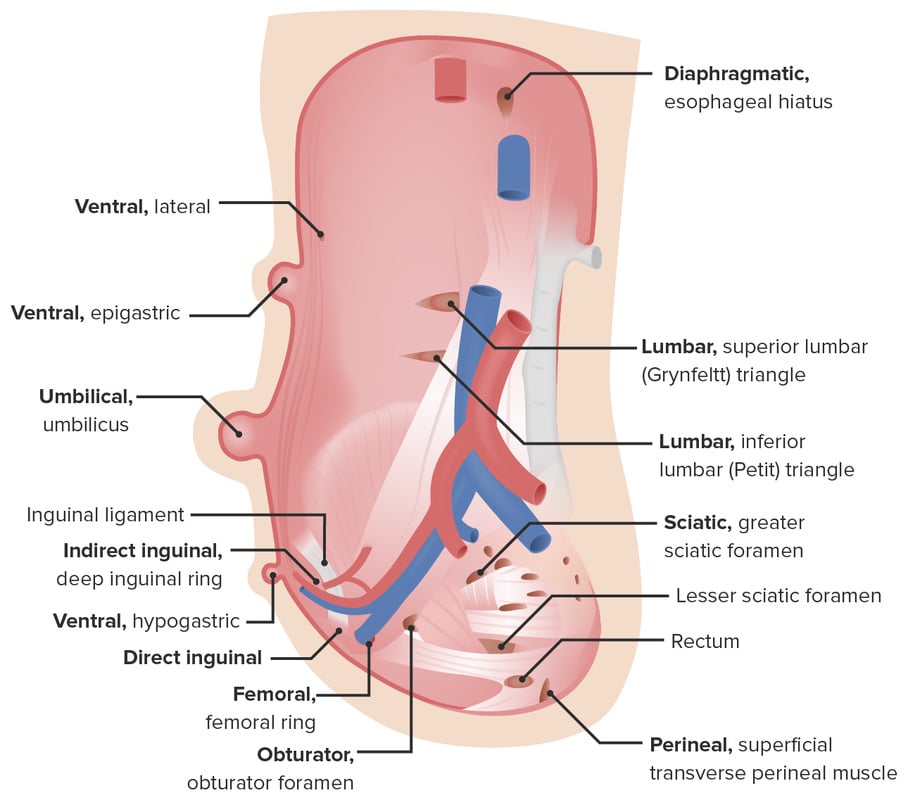
Hiatal (diaphragmatic) hernia: Involves protrusion of the stomach through the diaphragm via the esophageal hiatus. It can cause symptoms of GERD; acid reduction may suffice, although surgical repair can be used for more serious cases
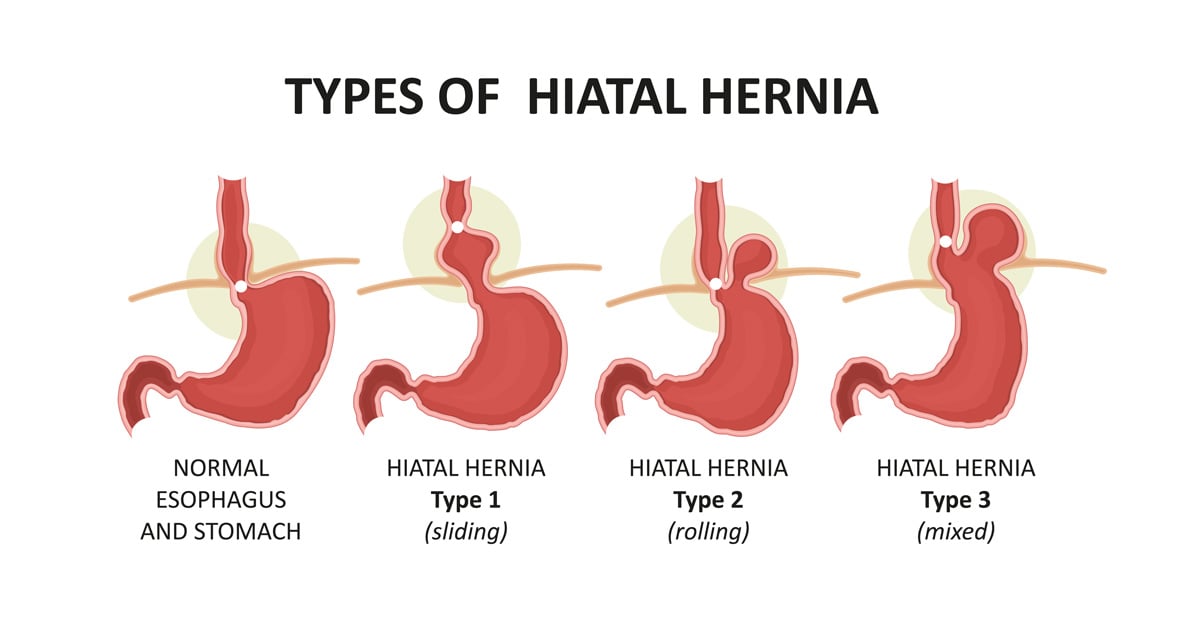
Types of Hiatal (Diaphragmatic) Hernias. Image by Adobe Stock.
Ventral hernia: Often from previous abdominal surgery, obesity. Abdominal mass noted at the site of a previous incision

Lateral ventral hernia
Umbilical hernia: Very common, generally congenital, and appears at birth. Many umbilical hernias resolve on their own and rarely require intervention. Refer to surgery if an umbilical hernia persists > 2 years of life

Umbilical hernia © Elena by Adobe Stock
Inguinal hernias:
- Indirect Inguinal Hernia (Most Common): Passage of intestine through the internal inguinal ring down the inguinal canal, may pass into the scrotum. Often congenital and will present before age one.
- Remember: Indirect goes through the Internal Inguinal Ring (an “I” for an “I”)

Indirect inguinal hernia on right side
- Direct Inguinal Hernia: Passage of intestine through the external inguinal ring at Hesselbach's triangle, rarely enters the scrotum

Direct inguinal hernia on the right
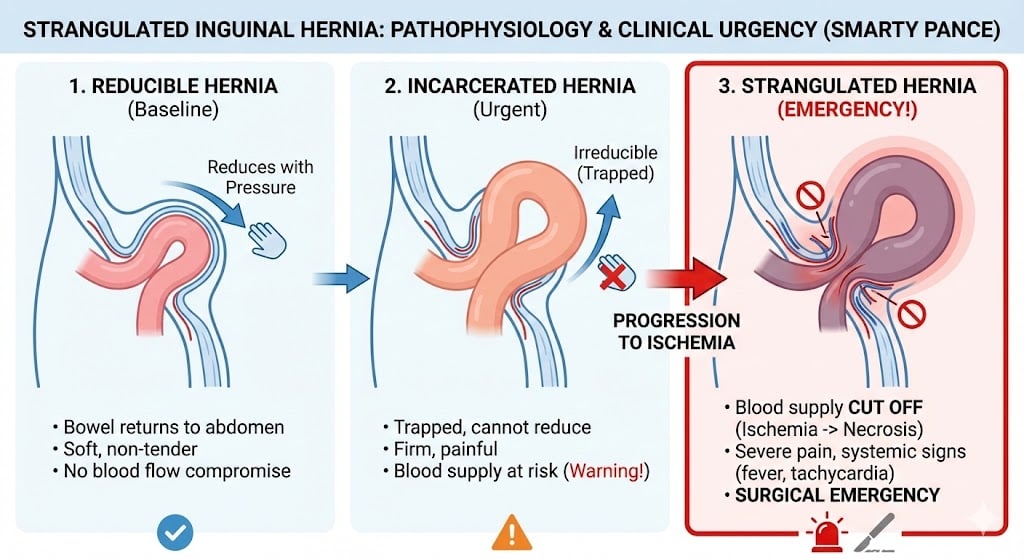
- Obstructed hernia: This is an irreducible hernia containing intestine that is obstructed from without or within, but there is no interference to the blood supply to the bowel.
- Incarcerated hernia: A hernia so occluded that it cannot be reduced by manipulation. It may or may not become strangulated. Incarcerated hernias are often surgical emergencies, and a surgeon should be consulted early.
- Strangulated hernia: A hernia becomes strangulated when the blood supply of its contents is seriously impaired
- Ultrasound - especially in a male child where other scrotal masses (hydrocele, varicocele) are considered
If the patient is otherwise well, refer non-urgently to surgery for definitive surgical repair
- If concerned about hernia incarceration or strangulation, refer immediately to surgery
 Osmosis Osmosis |
|
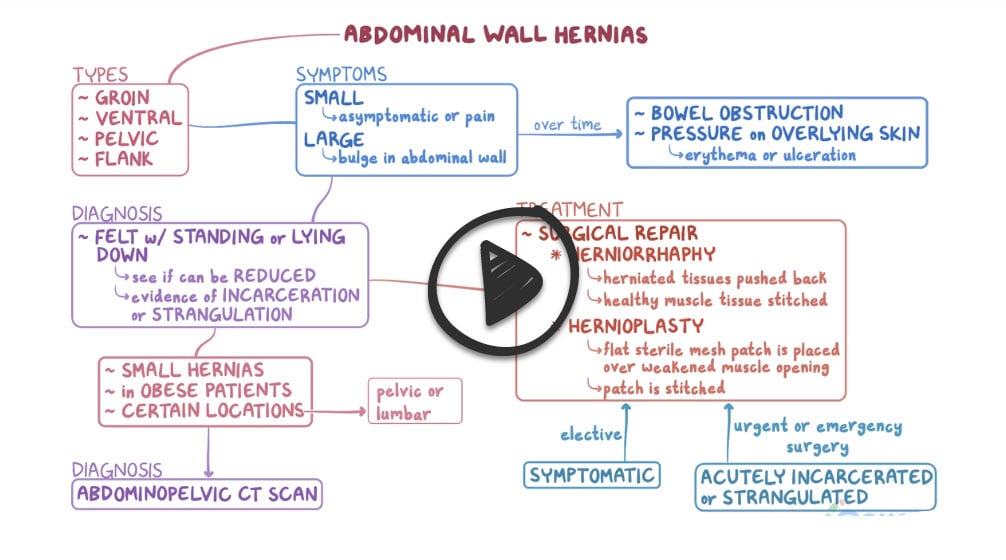 |

A hernia occurs when contents of the abdomen, usually a portion of the intestine, protrudes through an area of weakened muscle or tissue. Types of hernias include: hiatal, inguinal, femoral, umbilical, and incisional. If a hernia becomes strangulated, emergency surgery must be performed to restore blood flow and to prevent bowel necrosis.
Play Video + QuizHernia interventions
A hernia occurs when contents of the abdomen, usually a portion of the intestine, protrudes through an area of weakened muscle or tissue. Surgery can be performed to repair the hernia. Patients should be instructed to avoid activities, such as heavy lifting and sneezing after surgery, as these can increase intra-abdominal pressure
Play Video + QuizQuestion 1 |
Indirect inguinal hernia Hint: Indirect Inguinal Hernia (Most Common): Passage of intestine through the internal inguinal ring down the inguinal canal, may pass into the scrotum. Often congenital and will present before age one. | |
Direct inguinal hernia | |
Ventral hernia Hint: Ventral: Often from previous abdominal surgery, obesity. Abdominal mass noted at site of previous incision. | |
Hiatal hernia Hint: Hiatal (diaphragmatic): Involves protrusion of the stomach through the diaphragm via the esophageal hiatus. It can cause symptoms of GERD; acid reduction may suffice, although surgical repair can be used for more serious cases. |
Question 2 |
Direct inguinal hernia Hint: Passage of intestine through the external inguinal ring at Hesselbach triangle, rarely enters the scrotum | |
Indirect inguinal hernia | |
Umbilical hernia Hint: Very common, generally is congenital and appears at birth. Many umbilical hernias resolve on their own and rarely require intervention. Refer to surgery if an umbilical hernia persists >2 years of life | |
Ventral hernia Hint: Often from previous abdominal surgery, obesity. Abdominal mass noted at site of previous incision. |
Question 3 |
They are more common in women. Hint: See B for explanation | |
Has a low incidence of strangulation. | |
Cannot be controlled with a TRUSS. Hint: See B for explanation | |
accounts for about of 5% hernias in men. Hint: See B for explanation |
Question 4 |
Umbilical herniorrhaphy. Hint: Surgical treatment for complicated umbilical hernia before age 4-5years and complicated and uncomplicated hernia at age 4-5 years. | |
Conservative treatment. | |
Mayo's overlapping operation. Hint: Done to treat paraumbilical hernia. | |
None of the above. Hint: See B for answer |
Question 5 |
Chronic cough Hint: See D for explanation | |
Obesity Hint: See D for explanation | |
Heavy lifting Hint: See D for explanation | |
Diarrhea |
Question 6 |
Obstructed hernia Hint: This is an irreducible hernia containing intestine that is obstructed from without or within, but there is no interference to the blood supply to the bowel. | |
Strangulated hernia | |
Incarcerated hernia Hint: A hernia so occluded that it cannot be returned by manipulation, it may or may not become strangulated. | |
None of the above |
Question 7 |
Placing of intravenous line for rehydration and electrolyte correction. Hint: See D for explanation | |
Passage of nasogastric tube for decompression. Hint: See D for explanation | |
Administration of oxygen Hint: See D for explanation | |
Surgery |
|
List |
References: Merck Manual · UpToDate