| Topic | Key High-Yield Focus (Must-Know Points) |
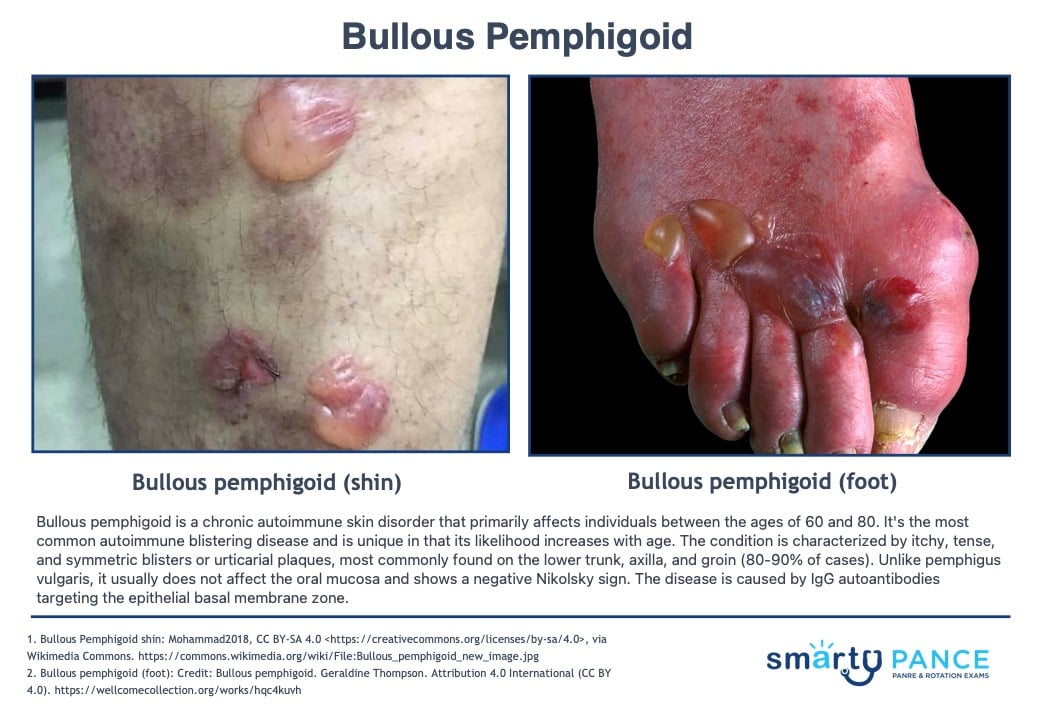
| 1. Bullous pemphigoid | Deep, tense bullae (unlike pemphigus vulgaris); negative Nikolsky sign; typically elderly patients; treated with systemic corticosteroids. |
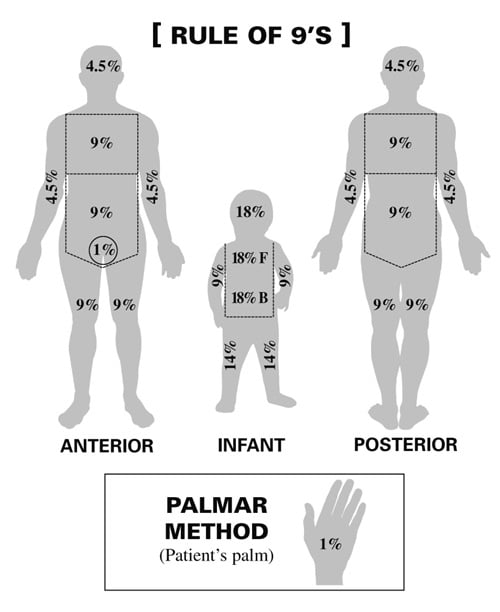
| 2. Burns | Parkland Formula: 4 mL × kg × %BSA (Body Surface Area); Rule of Nines; check for inhalation injury (soot in airway, singed nasal hairs) → early intubation. |
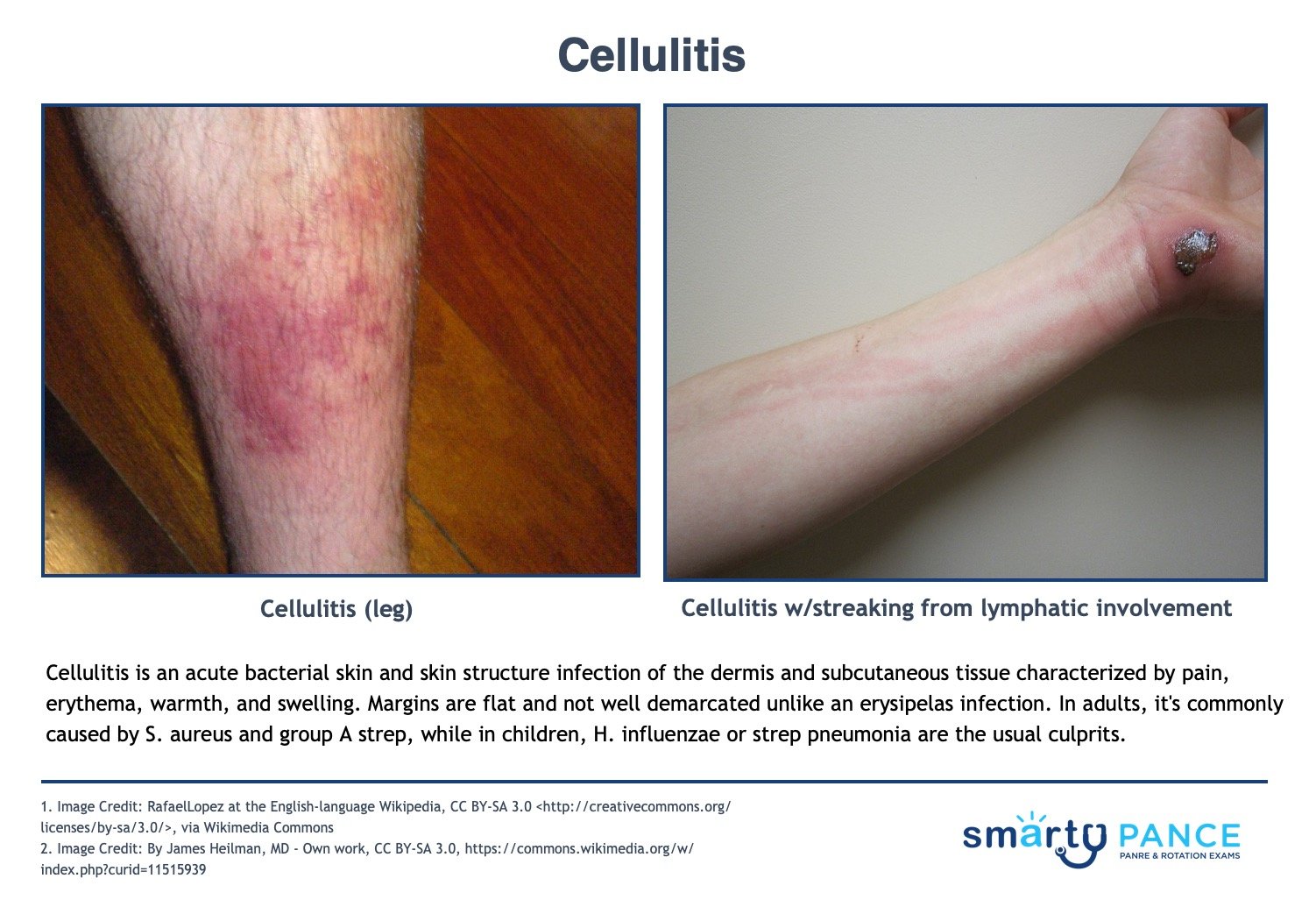
| 3. Cellulitis | Deep infection (dermis/subcutaneous); poorly demarcated borders; the most common cause is S. pyogenes or S. aureus; check for "tracking" or abscess. |
| 4. Dermatitis | Contact: Linear (poison ivy) or localized (nickel); Eczema: Flexor surfaces, "the itch that rashes," associated with asthma/allergies. |
| 5. Discharge | Focus on abscess management: Incision and Drainage (I&D) is primary; antibiotics only if systemic symptoms or significant cellulitis present. |
| 6. Drug eruptions | Exanthematous: Symmetric, morbilliform, starts 7–14 days after drug; Fixed drug eruption: Same spot every time drug is taken (often dusky red/purple). |
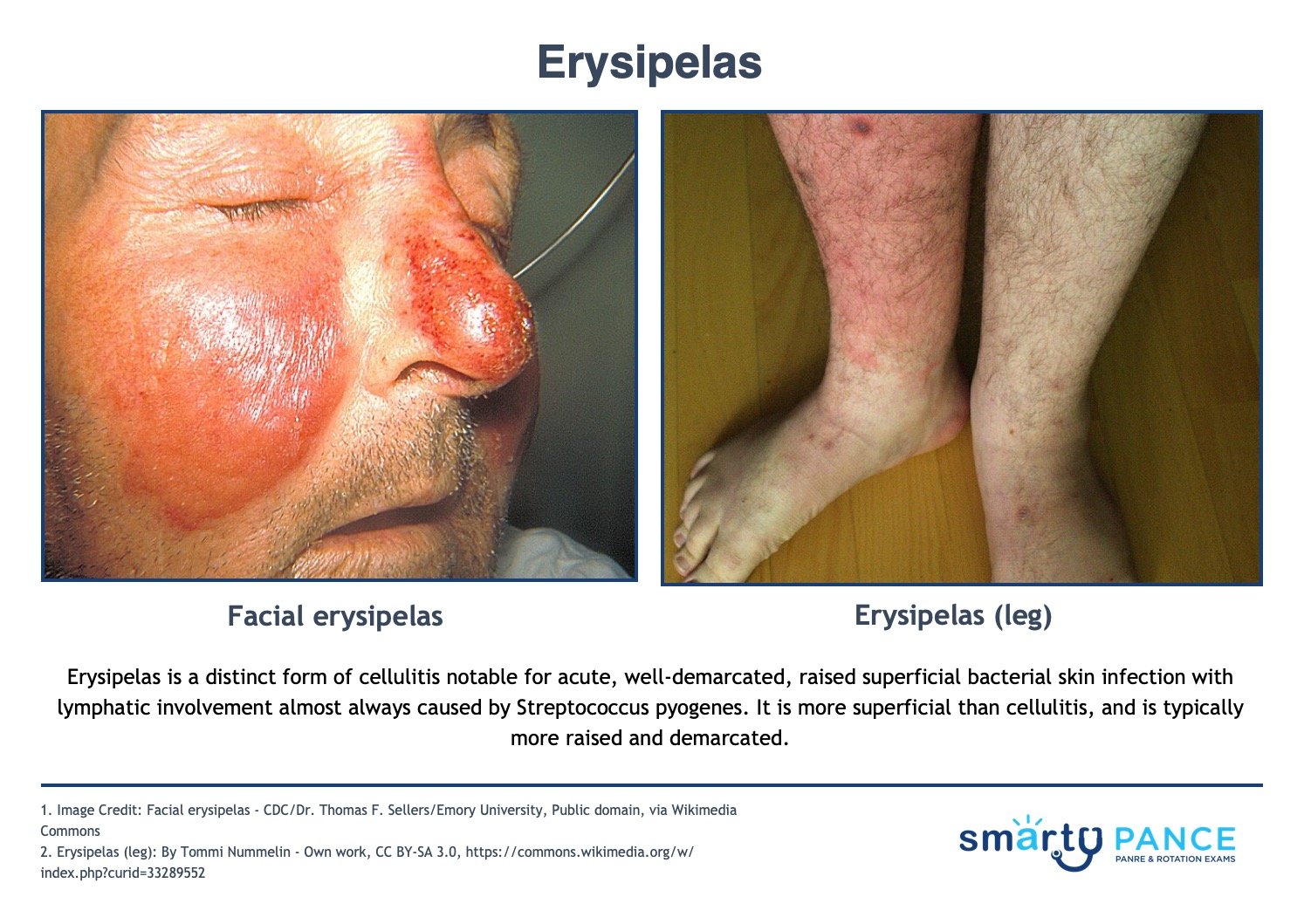
| 7. Erysipelas | Superficial infection; sharply demarcated raised borders; "butterfly" facial involvement common; caused by Group A Strep (S. pyogenes). |
| 8. Herpes zoster | Dermatomal distribution; does not cross midline; Hutchinson’s sign (tip of nose) → Ophthalmic emergency; treat with antivirals within 72 hours. |
| 9. Impetigo | Honey-colored crusts; common in kids; caused by S. aureus or S. pyogenes; treat with topical Mupirocin (Bactroban) or Cephalexin if bullous. |
| 10. Itching | Rule out systemic causes (renal/liver failure, lymphoma); focus on allergic reactions and primary skin disease (scabies, dermatitis). |
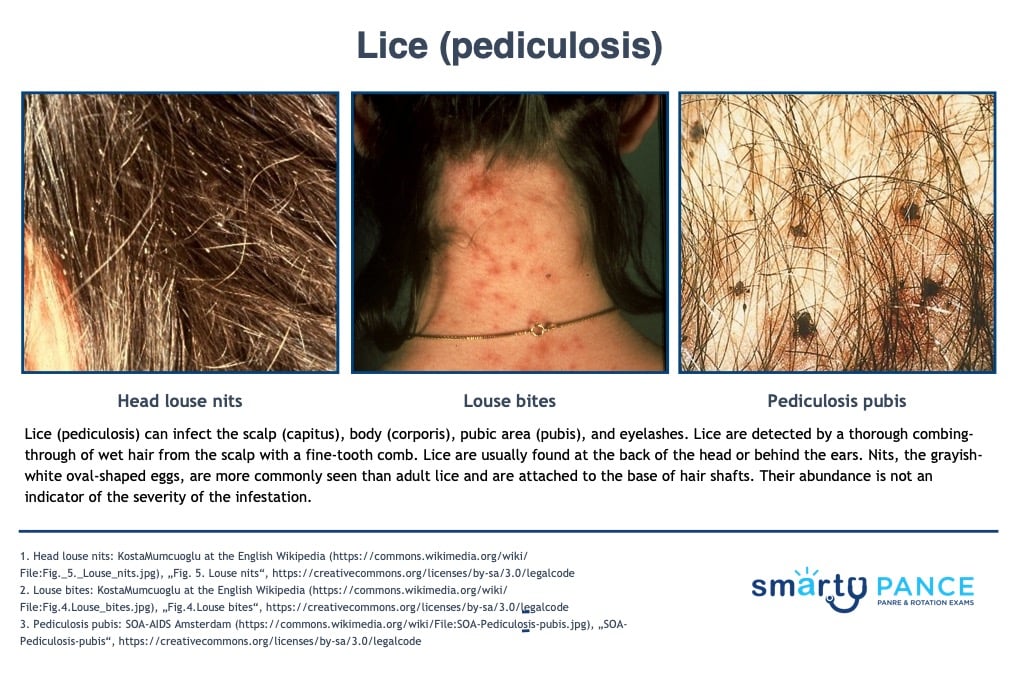
| 11. Lice | Nits (eggs) on hair shaft; treat with Permethrin; wash all bedding/clothing in hot water; treat household contacts. |
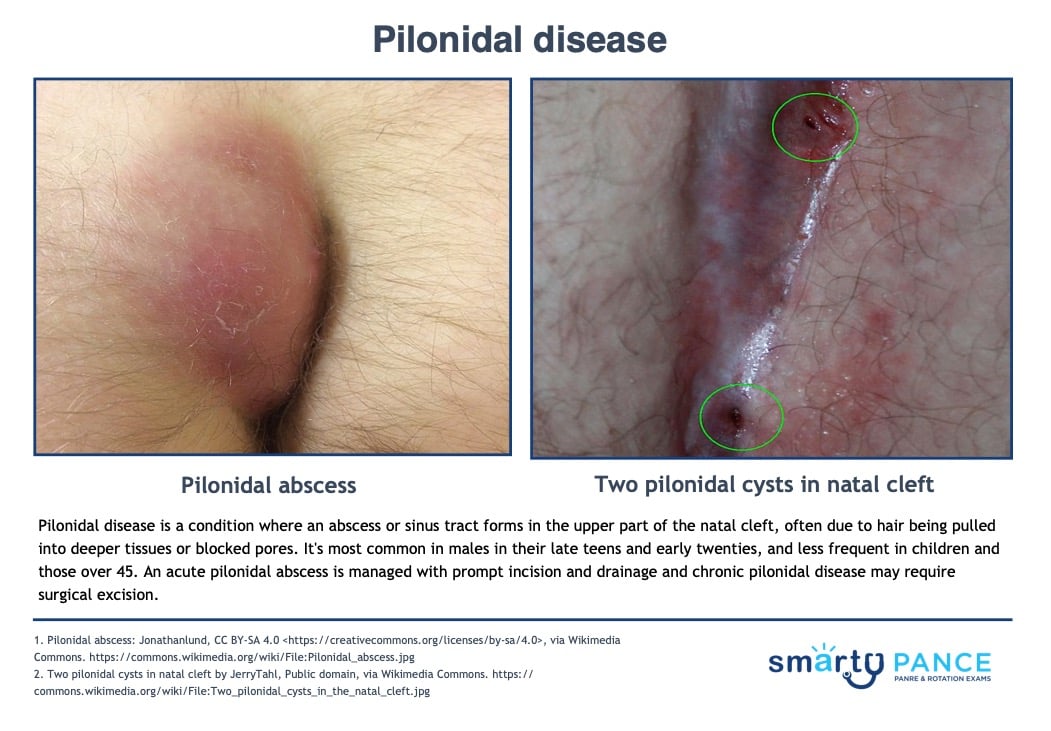
| 12. Pilonidal disease | Superior gluteal cleft; abscess/cyst; requires I&D in acute phase; definitive surgical excision for chronic sinus tracts. |
| 13. Pressure sores | Stage 1: Non-blanchable erythema; Stage 2: Partial thickness (blister); Stage 3: Full thickness (sub-q fat); Stage 4: Bone/muscle involvement. |
| 14. Rash | Focus on the "can't miss" list: Meningococcemia (non-blanching petechiae/purpura), Rocky Mountain Spotted Fever (starts on wrists/ankles). |
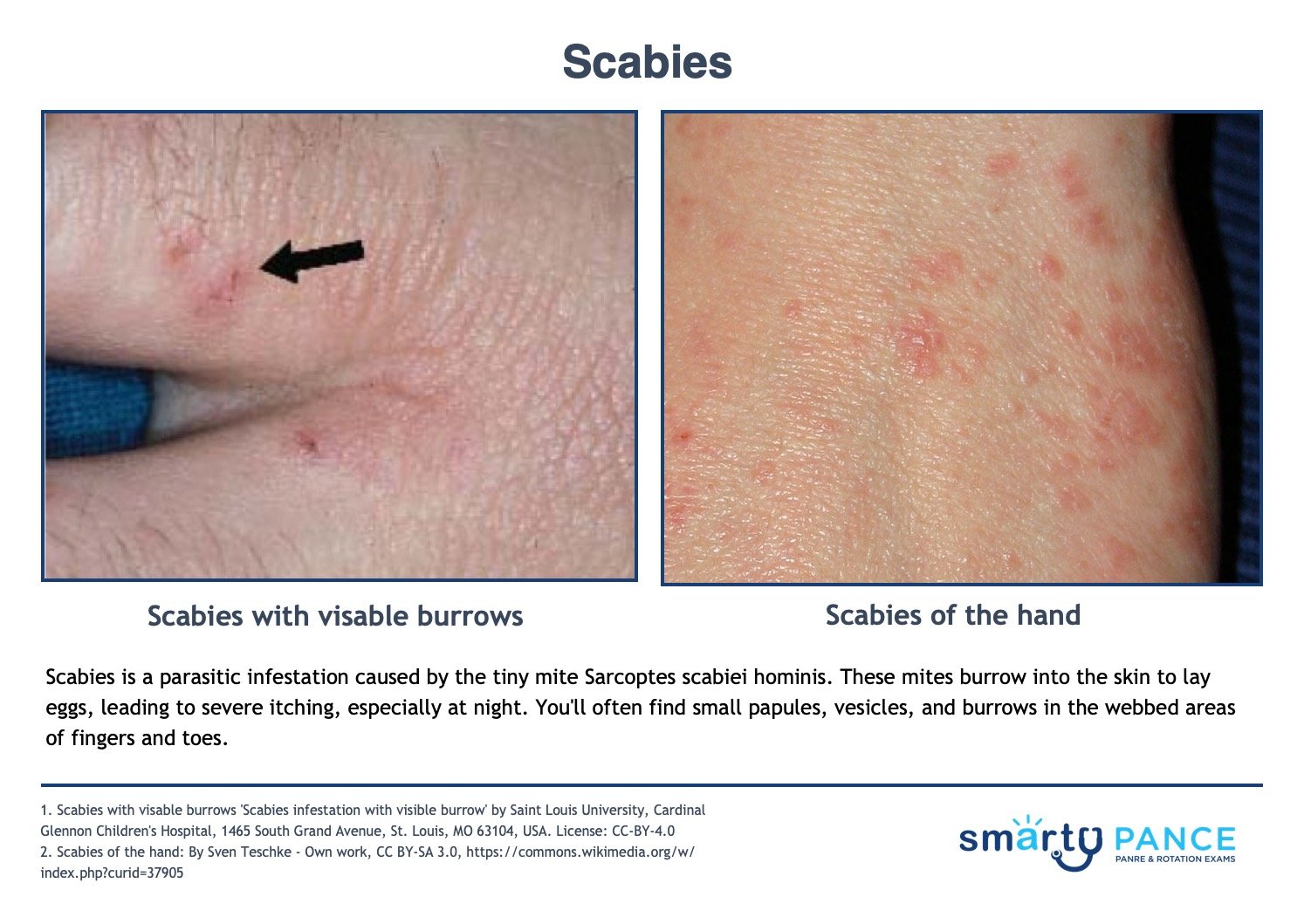
| 15. Scabies | Linear burrows in web spaces (fingers/toes), axilla, and groin; intense nocturnal pruritus; treat with Permethrin cream (neck down). |
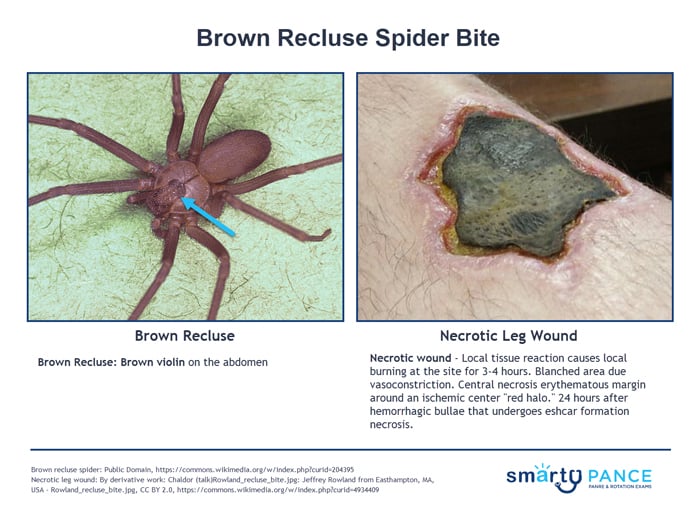
| 16. Spider bites | Brown Recluse: Local necrosis/eschar (red, white, and blue sign); Black Widow: Systemic muscle spasms, rigid abdomen, neurologic symptoms. |
| 17. SJS | <10% Body Surface Area (BSA) detachment; Positive Nikolsky sign; mucous membrane involvement; usually drug-induced (NSAIDs, Sulfa, Anticonvulsants). |
| 18. TEN | >30% BSA detachment; life-threatening; extreme skin sloughing; treat like a severe burn (fluid resuscitation, burn unit referral). |
| 19. Urticaria | Wheals/hives; blanchable and evanescent (individual lesions last <24 hrs.); check for angioedema or airway compromise (anaphylaxis). |
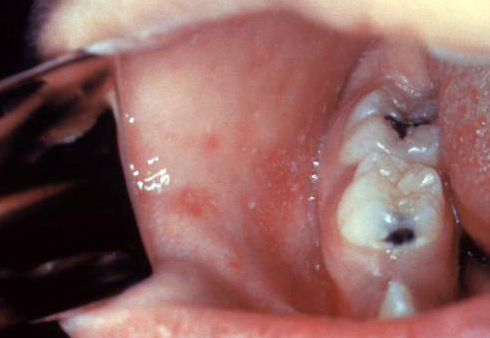
| 20. Viral exanthems | Measles: Cough/Coryza/Conjunctivitis + Koplik spots; Roseola: High fever then rash; Fifth Disease: Slapped cheek appearance. |
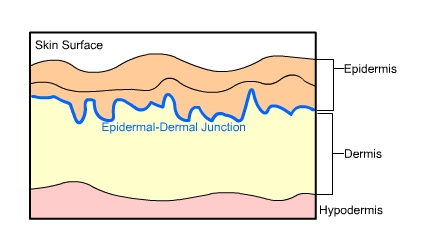
| Bullous pemphigoid | Patient will present as → a 75-year-old female who presents to the clinic with a large number of pruritic, tense, subepidermal bullae across her upper thighs. There was no mucosal involvement, a negative Nikolsky sign, and a skin biopsy showed subepidermal bullae filled with eosinophils and neutrophils. Bullous pemphigoid is a rare, chronic acquired autoimmune subepidermal blistering skin disorder caused by linear deposition of autoantibodies (IgG) against hemidesmosomes in the epidermal-dermal junction
Treat with systemic corticosteroids
|
| Lice | Patient will present as → a 9-year-old girl who is brought in by her mom, who noticed the child scratching her head at school pickup. She reports that this itchiness has gone on for around 1 week now. Her mom reports angrily that the school just notified them that several children had lice. Physical exam reveals several ovoid, grayish-white eggs < 1 cm away from the base of the hair shaft at the back of the head and behind the ears. She is given topical permethrin and counseled that she can still go to school. Pruritic scalp, body, or groin. Nits are observed as small white specs on the hair shaft
DX: Observation of lice and nits; nits = ovoid, grayish-white eggs TX: launder potential fomites such as sheets in hot water (> 131 F or 55 C)
View more images of pediculosis |
| Burns | Patient will present as → a 35-year-old male who was throwing some paint thinner on fire to get it going a little better when it splashed on him and caught his R arm and his R hip area on fire. He did not have pain right away and was not going to go to the hospital. He washed off the burnt areas because he had grease and oil on his hands and lower arm. The pain then started to get bad enough for him to have his wife take him to the ER. Body percentage:
Degree involvement:
Treatment: Monitor ABCs, fluid replacement, and sulfadiazine. Children with > 10% total body surface area and adults with > 15% total body surface area burns need formal fluid resuscitation
|
| Pilonidal disease |
|
| Cellulitis | ReelDx Virtual Rounds (Cellulitis)Patient will present as → a 64-year-old female with a 4 cm × 7 cm edematous, red, hot tender area on the left thigh. The lesion has gotten larger over the past 6 hours. She tells you she has also had a low-grade fever and some chills. On physical exam, there is a poorly demarcated 12cm red and tender plaque on her right calf. Some parts resemble an orange peel. There is a superficial cut in the middle of the plaque. An acute bacterial skin and skin structure infection of the dermis and subcutaneous tissue; characterized by pain, erythema, warmth, and swelling. Margins are flat and not well demarcated.
DX: Culture should be taken of all purulent wounds and followed up in 48 hours Treat mild cellulitis (MSSA)
Cat bites with augmentin or doxycycline if PCN allergic
Treat purulent or methicillin-resistant Staphylococcus aureus infection (MRSA) with
View more images of cellulitis |
| Pressure sores | Patient will present as → an 80-year-old bed-bound woman with a temperature of 104°F who you are called to see in the nursing home. The patient is disoriented and confused. On physical examination, the patient’s blood pressure is 110/ 80 mm Hg, and her pulse is 72 beats/ minute and regular. There is an 8 × 5 cm pressure ulcer over her sacrum. Also, there is a purulent, foul-smelling discharge coming from the ulcer. The sacrum and hip are most often affected. Reposition every 2 hours
Wound management by stage of the ulcer
Risk factors: age >65, impaired circulation, immobilization, undernutrition, incontinence DX: based on observation and staged according to classification TX: debridement ⇒ depends on the extent of necrosis; surgical closure may be necessary; vacuum-assisted closure uses negative pressure to reduce wound edema and remove debris/reduce bacterial load 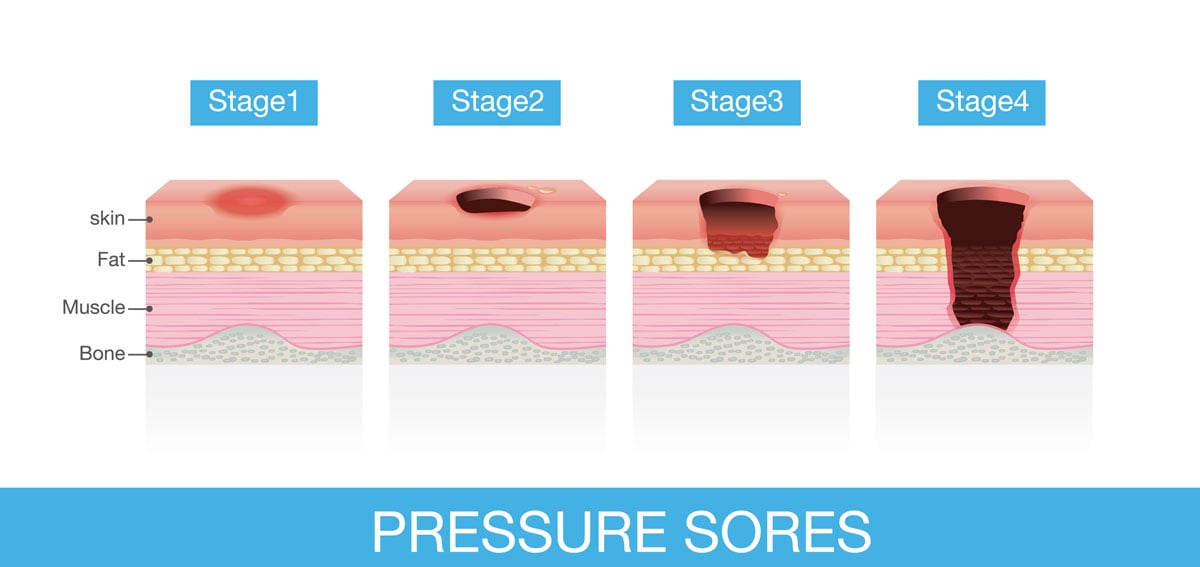 Pressure ulcer staging. Stage I, erythema; Stage II, breakdown of the dermis; Stage III, full-thickness skin breakdown; Stage IV, bone, muscle, and supporting tissue involved. |
| Dermatitis (eczema, contact) | Patient will present as → a 22-year-old female complaining of a rash around her mouth. She describes a feeling of mild burning or tension but denies pruritus. Examination reveals papulopustules on erythematous bases; the vermillion border is spared. A culture is negative 1. Contact dermatitis: well-demarcated erythema, erosions, vesicles
2. Atopic dermatitis: Pruritic, eczematous lesions, xerosis (dry skin), and lichenification (thickening of the skin and an increase in skin markings). Most common on flexor creases (e.g., antecubital and popliteal folds)
4. Seborrheic dermatitis (cradle cap): Erythematous, yellowish greasy scales, crusted lesions.
5. Perioral dermatitis: Young women. Papulopustular, plaques, and scales around the mouth.
View more images of dermatitis |
| Rash | Causes
Presentation:
Noninfectious rashes include eczema, contact dermatitis, psoriasis, seborrheic dermatitis, drug eruptions, rosacea, hives (urticaria), dry skin (xerosis), and allergic dermatitis. Infectious rashes can present with fever
Treatment
Pearls Rashes are a clue as to what the patient may be exposed to or what infection or systemic disease they may have it is a piece of information that can help to the diagnosis of the patient |
| Discharge | Breast/nipple discharge
GU
Other skin conditions
|
| Scabies | ReelDx Virtual Rounds (Scabies )Patient will present as → an 11-year-old male complaining of intensely itchy, painful, red streaks between his fingers and in the groin area. The patient reports that the itchiness seems to be worse at night. His best friend whom he had a sleepover this past weekend, is also having similar symptoms. Pruritic papules - S-shaped or linear burrows on the skin. Often located in web spaces of hands, wrists, and waist with severe itching (worse at night) DX: Microscopic observation of mites, eggs, or feces after a skin scrape TX: Treat with topical permethrin 5% - apply to the entire body and wash after 8-14 hours ⇒ repeat in one week (> 2 months old)
Pruritus may persist for 2-4 weeks after treatment
View more images of scabies |
| Drug eruptions | Patient will present as → a 17-year-old female with severe widespread red rash involving mainly the trunk and extremities one day after she took oral cefalexin suspension for a sore throat. An adverse cutaneous reaction in response to the administration of a drug, usually within the past 6 weeks
DX: clinical – consider bacterial, viral, underlying skin disease like cutaneous lymphoma TX: monitor for signs of impending cardiovascular collapse (anaphylaxis, DRESS (Drug Rash with Eosinophilia and Systemic Symptoms), SJS/TEN, extensive bullous reactions, generalized erythroderma)
View more images of drug eruptions |
| Spider bites | Brown Recluse:
Black Widow:
|
| Erysipelas | Patient will present as → a 19-year-old female with a painful rash on her left leg. She had a small bug bite in the same area about three weeks ago. Since then, the area has become red, painful, and hot. On physical exam, you note shiny, raised, indurated, and tender plaque-like lesions on the left leg. The redness is well-demarcated and hot to the touch. You send her home on penicillin. A distinct form of cellulitis notable for acute, well-demarcated, raised superficial bacterial skin infection with lymphatic involvement, almost always caused by Streptococcus pyogenes
DX: Wound culture and sensitivity
TX: Treat with antibiotics: regimen depends on location and severity
View more images of erysipelas |
| Stevens-Johnson syndrome | Patient will present as → a 60-year-old woman with a severe drug-induced reaction on both lower limbs with few lesions elsewhere in addition to mucosal involvement of the mouth of two days duration. The insulting drug was sulfonamide, and the onset of the rash was within 48 hours of taking the drug. The rash comprised bilateral symmetrical bullae on a background of erythematous macules and patches in addition to erosions and peeling. Stevens-Johnson syndrome is a rare, serious hypersensitivity complex that affects the skin and the mucous membranes. It's usually a reaction to a medication or an infection commonly caused by anticonvulsants and sulfa drugs!
DX: Skin biopsy shows necrotic epithelium DDX: erythema multiforme, viral exanthems, drug rash TX: Stop all offending medications, early admission to burn unit, manage fluid/electrolytes/nutrition, airway stability, eye care
View more images of SJS-TEN |
| Herpes zoster | ReelDx Virtual Rounds (Shingles)Herpes zoster (shingles): varicella reactivation causing a maculopapular rash along one dermatome Patient with herpes zoster (shingles) will present as → a 67-year-old male who presents to your clinic with a two-day history of a painful rash on his left flank radiating to his back. This was preceded by burning pain in the same region several days prior. The patient does not recall any history of childhood exanthems and is not up to date on his immunizations. Vital signs are stable. Physical exam reveals a maculopapular rash in a dermatomal distribution on the left flank and extending into the back.
Recombinant zoster vaccine (RZV, Shingrix) is recommended to prevent shingles in adults 50 years and older
|
| Toxic epidermal necrolysis | Patient will present as → a 60-year-old woman with a severe drug-induced reaction with extensive skin involvement covering > 30% of her body surface area. The insulting drug was anticonvulsant medication, and the onset of the rash was within 10 days of taking the drug. The rash comprised bilateral symmetrical bullae on a background of erythematous macules and patches in addition to erosion and peeling. On examination, her skin peels away in sheets when pressure is applied and rubbed. A rare, life-threatening skin condition that is usually caused by a reaction to drugs
DX: Confirm the diagnosis by biopsy (showing necrotic epithelium) TX: Early treatment decreases the often high mortality rate
|
| Impetigo | ReelDx Virtual Rounds (Impetigo)Patient will present as → a 5-year-old girl with crusting facial lesions present for 3 days. The mother reports that prior to the development of the facial lesions, her daughter was scratching at insect bites. Examination reveals a red facial rash with a golden “honey-colored crust” and pruritus. Child < 6 y/o complaining of non-painful, pruritic lesions on the face
Nonbullous impetigo: the most common form of impetigo caused by Staphylococcus aureus or Streptococcus pyogenes characterized by honey-colored crusts on the face and extremities
Bullous impetigo: Staphylococcus aureus impetigo that progresses rapidly from small to large flaccid bullae (newborns/young children) caused by epidermolytic toxin release. There is less lymphadenopathy and the trunk is more often affected; < 30% of patients
DX: The diagnosis is usually made clinically, but rarely a culture may be useful TX: topical mupirocin, dicloxacillin, cephalexin for more severe illness
|
| Urticaria | Patient will present as → a well-appearing 9-month-old male with a rash that comes and goes. According to the mother, citrus was recently added to the patient’s diet. On physical exam, you observe a widespread rash composed of blanchable, edematous, pink papules and wheals on the face, trunk, and lower extremities. The patient is started on PRN oral antihistamines for pruritus, and the mother is encouraged to eliminate citrus from his diet. The rash resolves within 72 hours. Urticaria (hives) is a skin rash triggered by a reaction to certain foods, medications, stress, or other irritants
DX: extensive lab testing not indicated; skin or IgE testing limited to the specific history of provoking allergen TX: Hives usually go away without treatment, but antihistamine medications are often helpful in improving symptoms
If anaphylaxis, give epinephrine: 0.3–0.5 mg. Use 1:1,000 dilution for IM route and 1:10,000 for IV route
|
| Itching | Presentation:
An uncomfortable, irritating sensation that creates an urge to scratch that can involve any part of the body. Common causes of this symptom:
Skin disorders
Systemic disorders
Treatment
Pearls: |
| Viral exanthems | Erythema infectiosum (fifth disease): Parvovirus B19 - "slapped cheek" rash on face - lacy reticular rash on extremities, spares palms and soles; resolves 2-3 weeks; supportive care/anti-inflammatories
Hand-foot-mouth disease: children < 10 years old caused by coxsackievirus type A virus-producing sores in the mouth and a rash on the hands, feet, mouth, and buttocks (watch video); usually clears in 10 days; tx = supportive / anti-inflammatories Measles (rubeola): The 4 C's - cough, coryza, conjunctivitis, and cephalocaudal spread
Rubella: 3-day rash; first appears on face, spreads caudally to trunk and extremities, and becomes generalized in 24 hours; cephalocaudal spread; teratogenic in 1st trimester (deafness, cataracts, TTP, mental retardation) Roseola (sixth disease): Herpesvirus 6 or 7, the only childhood exanthem that starts on the trunk and spreads to the face
|

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}