Patient will present as → a 25-year-old male presents for a routine exam. He has delayed puberty, gynecomastia, sparse body hair, and small testes. Labs show low morning testosterone with elevated LH/FSH. Karyotype: 47,XXY.
- DX: Primary (hypergonadotropic) hypogonadism
- TX: Lifelong testosterone replacement therapy (gel, injection, patch) to restore virilization, maintain bone density, and improve mood/energy. Fertility is usually impaired; assisted reproductive techniques may be considered.
Patient will present as → a 16-year-old girl is evaluated for primary amenorrhea and short stature. Exam shows webbed neck, wide-spaced nipples, and no breast development. Labs: low estradiol, elevated LH/FSH. Karyotype: 45,XO.
- DX: Primary ovarian failure (gonadal dysgenesis in Turner syndrome)
- TX: Estrogen replacement (with cyclic progesterone if uterus present) to induce/maintain secondary sexual characteristics, prevent osteoporosis, and support cardiovascular health. Fertility requires donor oocytes.
Patient will present as → a 45-year-old man on chronic opioids reports fatigue, low libido, and erectile dysfunction. Exam shows normal virilization but reduced testicular volume. Labs: low testosterone, low/normal LH/FSH; prolactin, thyroid, and cortisol are normal.
- DX: Secondary (hypogonadotropic) hypogonadism, opioid-induced
- TX: Address reversible causes (taper opioids if possible). If symptoms persist and fertility is not desired → testosterone replacement therapy. If fertility is desired → consider hCG or clomiphene citrate to stimulate endogenous testosterone/spermatogenesis.
Patient will present as → a 62-year-old man complains of decreased energy, reduced morning erections, and muscle loss. He has obesity, HTN, and diabetes. Labs: borderline low total T, low free T (↑ SHBG), normal LH/FSH.
- DX: Functional (late-onset) hypogonadism
- TX: Lifestyle modification first (weight loss, exercise, treat OSA, optimize comorbidities). If symptoms persist with confirmed low testosterone on ≥2 morning tests → consider testosterone replacement therapy, balancing benefits (sexual function, bone, muscle) vs risks (CV, prostate, erythrocytosis).
Patient will present as → a 22-year-old collegiate runner with low body weight and high training volume presents with secondary amenorrhea and infertility. Exam shows low BMI, no galactorrhea, and otherwise normal pubertal development. Labs: low estradiol, low/normal LH/FSH.
- DX: Secondary (hypothalamic) hypogonadism due to functional hypothalamic amenorrhea
- TX: Nutritional rehabilitation, weight restoration, and reduction of exercise intensity. Fertility can be achieved with ovulation induction using pulsatile GnRH or gonadotropins once energy balance is restored.
Hypogonadism = failure of the gonads (testes or ovaries) to produce sex hormones (testosterone/estrogen) ± impaired gametogenesis
Classifications
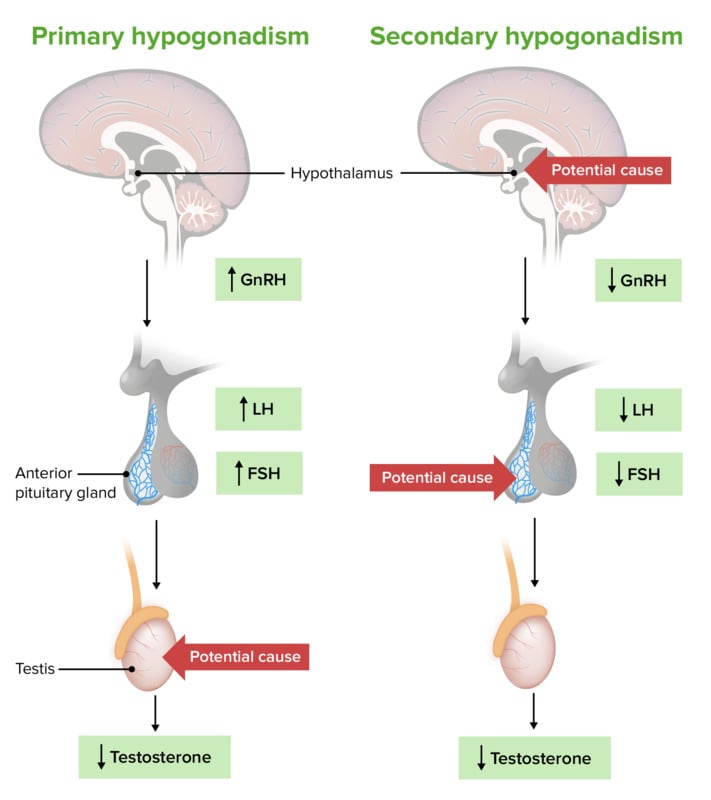
- Primary (hypergonadotropic): Gonadal failure → ↓ sex steroids, ↑ LH/FSH
- Secondary (hypogonadotropic): Hypothalamic or pituitary failure → ↓ LH/FSH → ↓ sex steroids
- Functional hypogonadism: Reversible suppression (illness, obesity, OSA, anorexia/athletic amenorrhea, medications) → ↓ testosterone in men or ↓ estradiol in women, with ↓/normal LH/FSH.
- Age-related hypogonadism: Aging with ↑ SHBG → ↓ free testosterone (men) or ↓ estradiol (women); LH/FSH usually normal.
Key Features
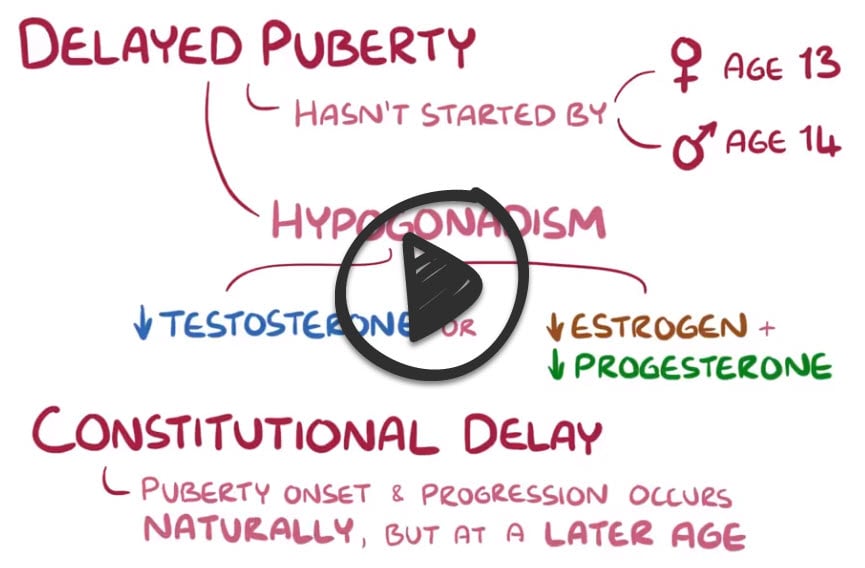
- Prepubertal onset: Delayed puberty, small testes/ovaries, tall stature (male), absent breast development (female).
- Postpubertal onset: ↓ libido, ED, infertility, fatigue, sarcopenia, osteoporosis (male); amenorrhea, hot flashes, infertility, vaginal dryness (female).
Comparison Table
| Type | Labs | Examples |
| Primary (gonadal failure) | ↓ Testosterone/Estradiol, ↑ LH/FSH | Klinefelter, Turner, orchitis, chemo/radiation, ovarian failure |
| Secondary (pituitary/hypothalamic failure) | ↓ Testosterone/Estradiol, ↓ or normal LH/FSH | Pituitary adenoma, Kallmann syndrome, opioids, infiltrative disease (hemochromatosis, sarcoid) |
| Functional / Age-related | Similar to secondary; no structural lesion | Obesity, chronic illness, aging, sleep apnea, anorexia/athletic amenorrhea |
The hypothalamic-pituitary-gonadal (HPG) axis in male hypogonadism
Adult Male Diagnosis
- Initial step: Correlate clinical features (low libido, ED, infertility, fatigue, decreased secondary sexual characteristics) with labs.
- Key labs:
- Morning total testosterone (age ≥18, 8–10 AM, fasting)
- LH/FSH → differentiates primary vs secondary
- Consider SHBG/free T if borderline
- Prolactin, TSH/free T4, AM cortisol, iron studies to screen for pituitary/hypothalamic disease
- Imaging:
- Pituitary MRI (if secondary suspected)
- Testicular US (if primary suspected)
- Fertility workup: Semen analysis if fertility concern
- Bone health: DEXA if osteoporosis or fractures present
- Algorithm:
- Low T + ↑ LH/FSH → Primary hypogonadism (testicular failure)
- Low T + ↓/normal LH/FSH → Secondary hypogonadism (pituitary/hypothalamic)
Diagnostic Algorithm for Male Hypogonadism (Adults)
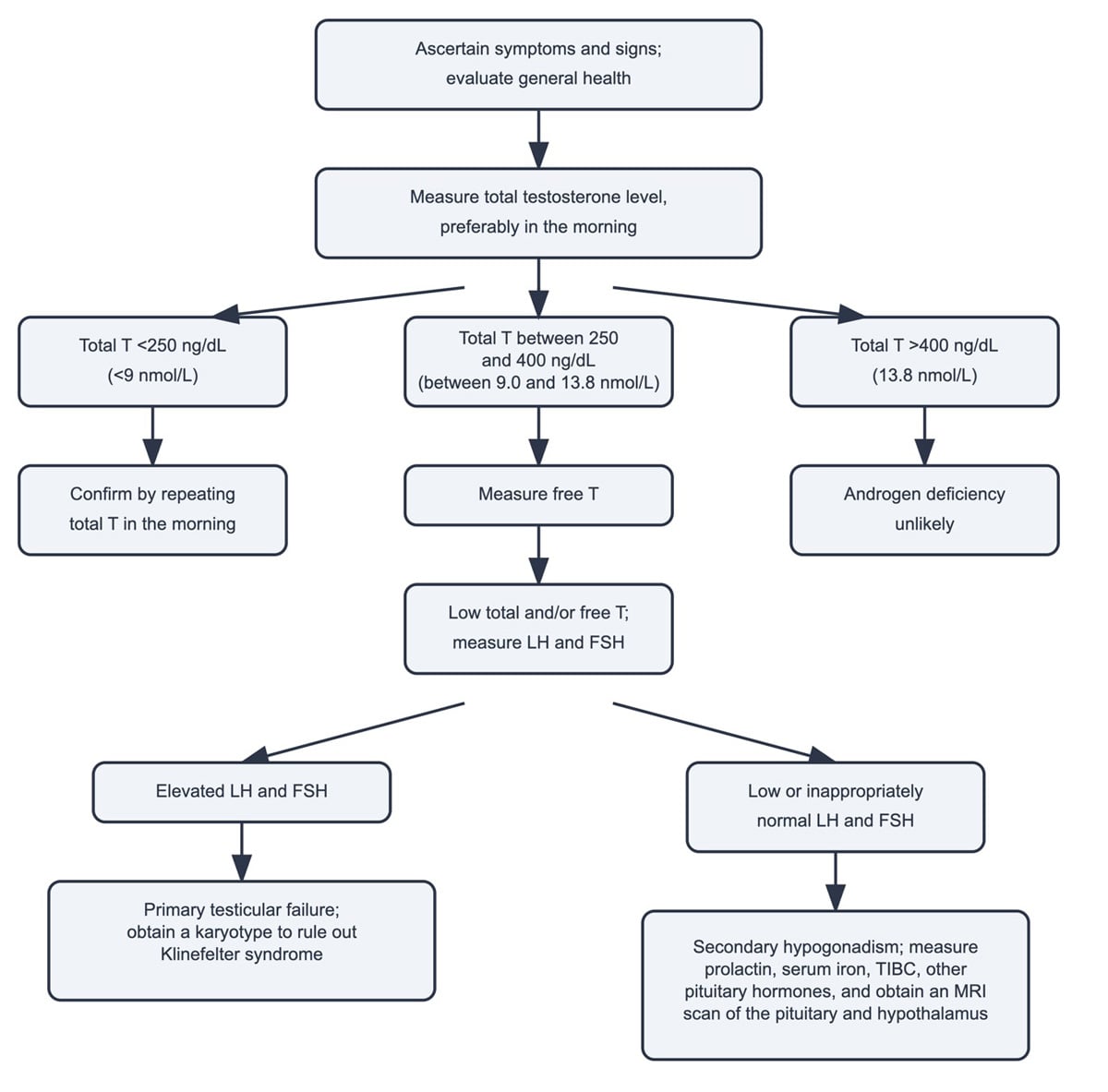
Adapted from UpToDate
Adult Female Diagnosis
- Initial step: Evaluate menstrual history, sexual development, menopausal symptoms, and infertility
- Key labs:
- Estradiol (low in hypogonadism)
- LH/FSH → differentiates primary vs secondary
- Pregnancy test (ALWAYS first in reproductive-age women)
- Prolactin, TSH/free T4, AM cortisol, and iron studies if secondary suspected
- Imaging:
- Pelvic ultrasound for ovarian morphology
- Pituitary MRI if secondary hypogonadism is suspected
- Fertility testing: Ovarian reserve testing (AMH, antral follicle count) if infertility is suspected
- Algorithm:
- Low estradiol + ↑ LH/FSH → Primary ovarian failure (eg, Turner, chemo/radiation, autoimmune)
- Low estradiol + ↓/normal LH/FSH → Secondary hypogonadism (eg, hypothalamic amenorrhea, pituitary disease)
Adolescent Diagnosis
- When to evaluate:
- Boys: No testicular enlargement (>4 mL) by age 14 or failure to progress
- Girls: No breast development by 13, no menarche by 15–16, or secondary amenorrhea
- Initial labs:
- Boys: LH, FSH, total testosterone
- Girls: LH, FSH, estradiol, pregnancy test
- Interpretation:
- ↑ LH/FSH + ↓ sex steroids → Primary (hypergonadotropic) hypogonadism
- Boys: Klinefelter, anorchia, testicular failure
- Girls: Turner, premature ovarian insufficiency
- ↓/normal LH/FSH + ↓ sex steroids → Secondary (hypogonadotropic) hypogonadism
- Functional (stress, eating disorder, excessive exercise)
- Pituitary/hypothalamic lesions (tumors, trauma, Kallmann syndrome)
- Normal labs + family history → Constitutional delay of puberty
- ↑ LH/FSH + ↓ sex steroids → Primary (hypergonadotropic) hypogonadism
- Next steps:
- Karyotype if primary suspected
- Pelvic/testicular ultrasound
- Pituitary MRI + endocrine panel if secondary suspected
Adult Male Treatment
Primary (testicular failure):
- Testosterone replacement therapy (TRT) if symptomatic and confirmed low T
- Forms: gel, patch, injection (enanthate/cypionate q1-2 weeks, undecanoate q10 weeks), pellets
- Fertility is rarely recoverable (spermatogenesis impaired)
Secondary (pituitary/hypothalamic):
- Treat underlying cause (eg, prolactinoma → dopamine agonist, iron overload → phlebotomy, tumors → surgery/radiation)
- Fertility desired: hCG or pulsatile GnRH to stimulate spermatogenesis
- Fertility not desired: TRT
Functional / Age-related hypogonadism:
- First-line: Lifestyle optimization (weight loss, treat OSA, manage chronic illness)
- If persistent symptoms + confirmed low T: Consider TRT, balancing benefits (sexual function, bone, muscle) vs risks (CV disease, erythrocytosis, prostate)
Monitoring:
- Recheck testosterone 2–3 months after starting therapy, then every 6–12 months
- Monitor hematocrit, PSA, lipids, and liver function
- Goal: maintain mid-normal testosterone (400–700 ng/dL), avoid supraphysiologic dosing
Adult Female Treatment
- Primary ovarian failure (eg, Turner, chemo/radiation):
- Hormone replacement therapy (HRT): estrogen + progestin (if uterus intact)
- Benefits: induces/maintains secondary sexual characteristics, protects bone and cardiovascular health
- Fertility: requires donor oocytes
- Secondary hypogonadism (pituitary/hypothalamic):
- Treat underlying cause (eg, prolactinoma → dopamine agonist, anorexia → nutritional rehab)
- Fertility desired → ovulation induction with pulsatile GnRH or gonadotropins
- Functional/age-related (menopause):
- Symptomatic management with individualized HRT (estrogen ± progestin depending on uterus)
- Focus: bone protection, vasomotor symptom relief, quality of life
- Monitoring:
- Ensure endometrial protection if uterus intact (always combine progestin with estrogen)
- Bone density q2 years if baseline osteoporosis
- Routine reassessment of risk–benefit for HRT
Adolescent Treatment
- Primary hypogonadism:
- Boys: Start low-dose testosterone (IM or transdermal), titrate gradually to adult replacement over 2–3 years → induces virilization, prevents osteoporosis
- Girls: Estrogen replacement (low dose, escalate gradually), add cyclic progesterone if uterus present → induces secondary sexual characteristics, protects bone
- Secondary hypogonadism (functional or structural):
- Functional hypothalamic amenorrhea (athletes, stress, anorexia): nutrition, weight restoration, stress reduction
- Structural (pituitary tumor, trauma): treat underlying lesion, then replace hormones as needed
- Constitutional delay of puberty:
- Reassurance if growth and puberty are simply a late family pattern
- Short-course low-dose sex steroids may be given for psychosocial support (eg, low-dose testosterone in boys, low-dose estrogen in girls)
 Osmosis Osmosis |
|
 |
Question 1 |
Normal gonadotropins (LH/FSH) and normal testosterone Hint: This finding would be more indicative of a normal hypothalamic-pituitary-gonadal axis and does not align with the patient's clinical presentation. | |
Elevated gonadotropins and low testosterone Hint: This pattern is suggestive of primary hypogonadism, where the problem lies in the testes, leading to decreased testosterone production and a compensatory increase in gonadotropins. | |
Elevated gonadotropins and high testosterone Hint: This finding is not typical of either primary or secondary hypogonadism and would prompt evaluation for other conditions. | |
Reduced gonadotropins and low testosterone | |
Reduced gonadotropins and high testosterone Hint: This is an unusual pattern and does not fit with secondary hypogonadism. High testosterone levels would not typically be seen in the setting of reduced gonadotropin levels unless there is an exogenous source of testosterone. |
Question 2 |
Primary testicular failure Hint: Typically presents with high gonadotropin levels, which is not indicated in the scenario. | |
Hyperprolactinemia Hint: Can cause hypogonadism, but there's no indication of prolactin elevation or related symptoms. | |
Secondary hypogonadism due to obesity and diabetes | |
Exogenous testosterone use Hint: Leads to suppressed gonadotropin levels, but there's no history of testosterone use. | |
Klinefelter syndrome Hint: A genetic cause of primary hypogonadism, usually diagnosed earlier in life. |
Question 3 |
Kallmann syndrome Hint: A form of secondary hypogonadism with low gonadotropin levels. | |
Primary hypogonadism | |
Secondary hypogonadism Hint: Characterized by low gonadotropin levels. | |
Androgen insensitivity syndrome Hint: Presents with female or ambiguous genitalia despite a male karyotype. | |
Prolactinoma Hint: Would typically present with hyperprolactinemia and possibly low gonadotropin levels. |
Question 4 |
Testosterone gel | |
Oral testosterone undecanoate Hint: While this is a form of testosterone replacement, it is not typically the first choice due to concerns about liver toxicity and less stable testosterone levels compared to gels or injections. | |
High-dose intramuscular testosterone enanthate Hint: Parenteral testosterone can be used in hypogonadism treatment, but high doses are not usually the initial approach due to the risk of erythrocytosis and other side effects. Dosing should aim for mid-normal serum testosterone levels. | |
Clomiphene citrate Hint: This is used primarily for treating infertility due to hypogonadotropic hypogonadism and is not the standard treatment for typical hypogonadism with low testosterone levels. | |
Transdermal estrogen patch Hint: Estrogen therapy is not used in the treatment of male hypogonadism. Testosterone replacement is the appropriate therapy for hypogonadal men. |
|
List |
References: Merck Manual · UpToDate