The NCCPA™ PANCE Cardiology System Content Blueprint includes two topics related to lipid disorders
{kind=link}
{kind=link}
{kind=link}
Screening Guidelines (2026 ACC/AHA)
👉 Click here for a summary of the new AHA guidelines (click here)
- Universal baseline: Adults should have a lipid profile beginning in young adulthood (about age 19 to 20), repeated about every 5 years in low-risk individuals
- Higher-risk patients: Screening and follow-up should be performed more frequently based on age, ASCVD risk, and treatment goals
- Earlier screening is appropriate in patients with a family history of premature ASCVD or familial hypercholesterolemia (FH)
- Lp(a) screening: Measure Lipoprotein(a) [Lp(a)] at least once in adulthood to refine cardiovascular risk — especially with a strong family history of premature ASCVD.
- An Lp(a) ≥ 125 nmol/L (or ≥ 50 mg/dL) is associated with increased ASCVD risk; Lp(a) ≥ 250 nmol/L confers substantially higher risk. Lifestyle changes minimally affect Lp(a), so repeat testing is generally not needed
The 2026 guidelines replace the old Pooled Cohort Equations (PCE) with the AHA PREVENT™ equations for 10- and 30-year ASCVD risk assessment in adults aged 30–79 years.
Key features of PREVENT™:
- Includes eGFR (estimated glomerular filtration rate) as a risk variable
- Removes race-based variables
- Generally yields slightly lower risk estimates than the old PCE
10-Year Risk Categories:
- High Risk: ≥ 10% → statin therapy is recommended
- Intermediate Risk: 5% to < 10% → statin therapy is recommended
- Borderline Risk: 3% to < 5% → statin therapy may be considered after risk discussion
- Low Risk: < 3% → lifestyle therapy is recommended; statin is generally not indicated unless LDL-C ≥ 160 mg/dL or 30-year risk is elevated
| Risk Tier | 10-Year PREVENT™ | Action | Statin Intensity | LDL-C Goal |
| Low | < 3% | Lifestyle counseling; statin generally not indicated unless LDL-C ≥ 160 mg/dL or 30-year risk ≥ 10% | Moderate (if treating) | < 100 mg/dL |
| Borderline | 3% to < 5% | Lifestyle counseling + risk-benefit discussion; evaluate risk enhancers; consider CAC if uncertain | Moderate (if treating) | < 100 mg/dL; non-HDL-C < 130 mg/dL |
| Intermediate | 5% to < 10% | Start statin therapy; consider CAC if uncertainty remains about intensity | Moderate-to-High | < 100 mg/dL; non-HDL-C < 130 mg/dL |
| High | ≥ 10% | Start high-intensity statin; add ezetimibe, PCSK9i, or bempedoic acid if goals are not met | High-Intensity | < 70 mg/dL; non-HDL-C < 100 mg/dL |
⭐ These groups receive lipid-lowering therapy (LLT) regardless of calculated PREVENT™ risk:
(1) Clinical ASCVD, (2) LDL-C ≥ 190 mg/dL, and (3) age 40–75 with diabetes, CKD stage ≥ 3, or HIV on stable antiretroviral therapy.
Only clinical ASCVD qualifies as secondary prevention — the other groups remain primary prevention despite high risk.
- Clinical ASCVD = prior MI, angina, coronary revascularization, ischemic stroke/TIA, PAD, or aortic atherosclerotic disease
DX: Diagnostic Evaluation
Screening may include total cholesterol alone, total and HDL cholesterol, or LDL and HDL cholesterol levels. If LDL-C cannot be calculated (triglycerides ≥ 400 mg/dL), direct LDL-C or non-HDL-C should be used.
- Apolipoprotein B (ApoB) may be used to assess residual ASCVD risk in patients with cardiovascular-kidney-metabolic syndrome, type 2 diabetes, high triglycerides, or established CVD who have reached LDL-C and non-HDL-C goals. ApoB may better represent the true atherogenic particle burden.
Four Groups Most Likely to Benefit from Lipid-Lowering Therapy (2026 Update)
- Secondary Prevention: Patients with any form of clinical atherosclerotic cardiovascular disease (ASCVD) (ACS, MI, stable angina, coronary revascularization, stroke/TIA, PAD)
- Severe Hypercholesterolemia: Primary LDL-C ≥ 190 mg/dL — assess for familial hypercholesterolemia and secondary causes
- Diabetes / CKD / HIV: Age 40–75 years with diabetes, CKD stage ≥ 3, or HIV
- Primary Prevention (Risk-Based): Adults age 30–79 with a PREVENT™ 10-year ASCVD risk ≥ 5% (intermediate or higher); statin consideration begins at ≥ 3% (borderline)
⭐ NEW (2026): Consider initiating lipid-lowering therapy starting at age 30 for individuals with heterozygous familial hypercholesterolemia (FH), LDL-C ≥ 160 mg/dL plus a strong family history of ASCVD, or a high 30-year PREVENT™ risk. The central philosophy of the 2026 guidelines is "earlier and lower for longer."
Use the AHA ASCVD Risk Calculator (PREVENT™) for risk assessment.
Unlike the 2018 guidelines (which had no specific LDL-C targets), the 2026 guidelines restore numerical LDL-C goals:
- Secondary Prevention — Very High Risk (≥2 events OR 1 event + comorbidities): LDL-C < 55 mg/dL
- Secondary Prevention — Not Very High Risk (1 ASCVD event, minimal comorbidities): LDL-C < 70 mg/dL
- Primary Prevention — FH, LDL-C ≥ 190 mg/dL, or High Risk (≥ 10%): LDL-C < 70 mg/dL
- Primary Prevention — coronary artery calcium (CAC) ≥ 1000 AU: LDL-C < 55 mg/dL (treat as very high risk)
- Primary Prevention — Intermediate Risk (5–10%): LDL-C < 100 mg/dL
- Borderline/Low Risk (< 5%): LDL-C < 100 mg/dL (optimal goal if treating)
Risk Enhancers ("Tie-Breakers")
For patients in the Borderline (3–< 5%) or Intermediate (5–< 10%) risk groups where the decision to treat is uncertain, the presence of any of the following should favor initiating or intensifying statin therapy:
- Family History: Premature ASCVD (first-degree relative: men < 55, women < 65)
- Lp(a) ≥ 50 mg/dL (or ≥ 125 nmol/L)
- Chronic Inflammatory Conditions: Psoriasis, rheumatoid arthritis, lupus, HIV/AIDS
- Chronic Kidney Disease: eGFR 15–59 mL/min/1.73m²
- Metabolic Syndrome: Elevated waist circumference, high TG, low HDL, HTN, elevated fasting glucose
- ApoB ≥ 130 mg/dL or elevated non-HDL-C
- South Asian ancestry
When risk remains uncertain after applying PREVENT™ and risk enhancers, CAC scoring should be considered to guide the decision to initiate or withhold statin therapy:
- Recommended for men ≥ 40 years and women ≥ 45 years with borderline or intermediate PREVENT™ risk
- CAC = 0: Statin therapy may reasonably be deferred (unless diabetes, smoking, or strong family history)
- CAC 1–99: Statin therapy is reasonable
- CAC ≥ 100 or ≥ 75th percentile for age/sex/race: Statin therapy is indicated
- CAC ≥ 1000 AU: LDL-C target < 55 mg/dL (treat as very high risk)
TX: Statin Intensity Therapy
| INTENSITY | LDL-C LOWERING | MEDICATIONS & DOSAGES |
| High Intensity | ≥ 50% | Atorvastatin (Lipitor) 40–80 mg Rosuvastatin (Crestor) 20–40 mg |
| Moderate Intensity | 30% to 49% | Atorvastatin 10–20 mg Rosuvastatin 5–10 mg Simvastatin (Zocor) 20–40 mg Pravastatin (Pravachol) 40–80 mg Lovastatin (Mevacor) 40 mg Pitavastatin (Livalo) 2–4 mg Fluvastatin XL (Lescol XL) 80 mg |
| Low Intensity | < 30% | Simvastatin 10 mg Pravastatin 10–20 mg Lovastatin 20 mg Pitavastatin 1 mg |
⭐ NEW (2026): Non-Statin Add-On Therapy — Expanded Roles
When LDL-C goals are not met with maximally tolerated statin therapy, add non-statin agents in a stepwise fashion:
| Agent | Mechanism | LDL-C Reduction | Class / Notes |
| Ezetimibe (Zetia) | Inhibits intestinal cholesterol absorption | ~18–25% | First-line add-on to statin |
| Bempedoic Acid (Nexletol) | Inhibits ATP-citrate lyase (upstream of HMG-CoA reductase); activated only in the liver — no myopathy risk, no TG-lowering effect | ~18–25% | NEW — expanded role in 2026; useful in selected high-risk patients who need further LDL lowering and in statin-intolerant patients |
| PCSK9 Inhibitors Evolocumab (Repatha) Alirocumab (Praluent) SQ every 2–4 weeks |
Monoclonal antibody blocks PCSK9, increasing LDL receptor recycling | 50–60% | Major add-on option for high-risk patients not at goal; high cost and prior authorization often required |
| Inclisiran (Leqvio) SQ every 6 months |
siRNA targeting PCSK9 mRNA — reduces hepatic PCSK9 production | ~50% | NEW — Class IIa; useful for patients unable to access or tolerate PCSK9 monoclonal antibodies or who prefer less frequent dosing |
| Bile Acid Sequestrants Cholestyramine (Questran) Colesevelam (Welchol) |
Binds bile acids in gut, increasing hepatic LDL receptor upregulation | ~15–18% | Side effects: constipation, bloating; avoid with hypertriglyceridemia (can raise TG) |
Medications and Key Side Effects
- Statins: Side effects: Myalgias, elevated LFTs, rhabdomyolysis (check CK if myalgias; tea-colored urine = rhabdomyolysis); contraindicated in pregnancy
- Fibrates: Side effects: Gallstones, myopathy (especially with gemfibrozil + statin); fenofibrate preferred over gemfibrozil when combining with statins
- Niacin: Side effects: Flushing (treat with aspirin 30 min before dose); worsening glycemic control — no longer routinely recommended
- Bile acid sequestrants (Cholestyramine): Side effects: Constipation, bloating
- Ezetimibe: Side effects: Generally well-tolerated; rare myalgias
- PCSK9 inhibitors: Side effects: Injection site reactions, generally well-tolerated
- Bempedoic acid: Side effects: Gout (raises uric acid), avoid with simvastatin > 20 mg
Board Pearls for Hypercholesterolemia
- “The Three Numbers”: Memorize 55 / 70 / 100 — the LDL-C targets for very high-risk secondary prevention, high-risk primary prevention / severe hypercholesterolemia, and intermediate-risk primary prevention, respectively
- “Earlier and Lower for Longer” — the central message of the 2026 guidelines. Consider starting therapy at age 30 in FH or high long-term risk
- Statin Choice: Atorvastatin and Rosuvastatin are the high-intensity “big guns”
- PREVENT™ thresholds: ≥ 5% (intermediate) = statin recommended; ≥ 3% (borderline) = statin consideration after risk discussion
- Lp(a): If a young patient has an MI with “normal” LDL, check Lp(a)
- Myalgias on statin? Check CK. Tea-colored urine? Think rhabdomyolysis
- Pregnancy: Statins are contraindicated — stop before conception
- Bempedoic acid is a useful option when additional LDL lowering is needed, especially in statin-intolerant patients
- Inclisiran is dosed only twice a year
- CAC = 0 in a low/borderline risk patient? It is reasonable to defer statin therapy
- CAC ≥ 1000 AU = treat like very high risk → LDL-C target < 55 mg/dL
- Only clinical ASCVD = secondary prevention. LDL-C ≥ 190 mg/dL, diabetes, CKD, and HIV are still primary prevention groups
Adults should have universal lipid screening beginning in young adulthood and repeated about every 5 years in low-risk patients.
- Normal – < 150 mg/dL
- Mild to moderate hypertriglyceridemia – 150 to 499 mg/dL
- Moderate to severe hypertriglyceridemia – 500 to 999 mg/dL
- Severe hypertriglyceridemia – ≥ 1000 mg/dL
Normal NON-FASTING triglyceride levels are generally considered below 200 mg/dL
Clinical Manifestations of Hypertriglyceridemia
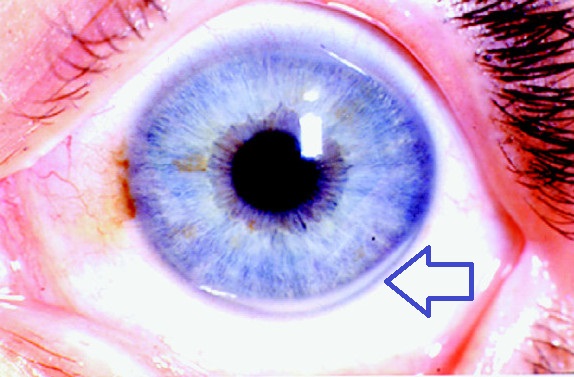
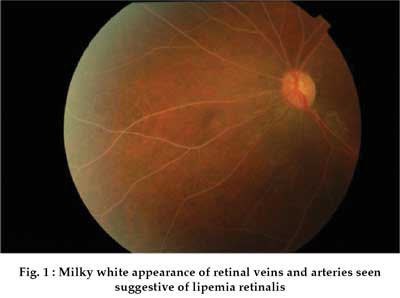
- Moderate to severe hypertriglyceridemia (> 500 mg/dL) may cause pancreatitis, eruptive xanthomas, and lipemia retinalis
- Triglycerides > 2000 mg/dL can cause chylomicronemia syndrome: recurrent abdominal pain, nausea, vomiting, and pancreatitis
- Eruptive xanthomas are 1–3 mm yellow papules typically seen on the back, chest, and proximal extremities
- Palmar xanthomas (yellow palmar creases) are seen in type III hyperlipidemia
{kind=link}
{kind=link}
- Beta-blockers
- High-dose thiazide diuretics/chlorthalidone
- Corticosteroids
- Atypical antipsychotics (clozapine, olanzapine)
- Protease inhibitors (HIV medications)
- Oral contraceptives (high estrogen content)
- Retinoids (isotretinoin)
- Immunosuppressants (cyclosporine)
- Tamoxifen
Treatment Goals
- The primary reasons to treat hypertriglyceridemia are to prevent pancreatitis (TG > 500 mg/dL) and reduce ASCVD risk
- Triglyceride level should be reduced to < 500 mg/dL to prevent pancreatitis
- Management of ASCVD risk focuses primarily on lowering LDL-C and non-HDL-C, not TG alone
Treatment: Therapeutic Lifestyle Changes (TLC) — First Line for All Patients
- Low-fat, carbohydrate-controlled diet: Reduce simple sugars and high-fructose foods; target < 6% added sugar calories; increase omega-3-rich fish (salmon, mackerel, herring) ≥ 2 servings/week
- Alcohol: Limit or eliminate (avoid completely for TG > 500 mg/dL or history of pancreatitis)
- Weight loss: 5–10% body weight reduction significantly lowers TG
- Aerobic exercise: At least 150 min/week moderate intensity (or 75 min vigorous)
- Address secondary causes: Optimize glycemic control in diabetes; treat hypothyroidism; review medications
Pharmacologic Treatment by TG Level
| Therapy | TG Reduction | LDL Effect | HDL Effect | Key Side Effects |
| Statins Atorvastatin 40–80 mg Rosuvastatin 20–40 mg (high intensity preferred) |
20–44% (up to 44% with high-intensity at high TG baseline) |
18–55% reduction | 5–15% increase | Myopathy, rhabdomyolysis, ↑ LFTs; first-line for ASCVD risk reduction |
| Fibrates *Fenofibrate (TRICOR) 145 mg daily — PREFERRED Gemfibrozil (Lopid) 600 mg BID |
40–60% | Mild increase | 15–25% increase | Rhabdomyolysis (especially gemfibrozil + statin); hepatotoxicity; nephrotoxicity (fenofibrate); ↑ warfarin effect |
| Marine Omega-3 Fatty Acids *Icosapent ethyl (Vascepa) 2 g BID — PREFERRED for high ASCVD risk Omega-3 ethyl esters (Lovaza) 4 g daily — acceptable for lower ASCVD risk |
20–50% | Mild increase (less with EPA-only; more with DHA-containing) |
5–10% increase | GI upset, fishy aftertaste; ↑ atrial fibrillation risk — use fibrates instead in patients with paroxysmal AFib; avoid in TG > 880 mg/dL (fat restriction essential) |
| ⭐ NEW: APOC3 Inhibitors Olezarsen (Tryngolza) 80 mg SQ monthly — FDA-approved for FCS Plozasiran 25 mg SQ quarterly — FDA-approved for FCS |
40–85% (olezarsen) ~78–80% (plozasiran) |
Minimal LDL effect; reduces non-HDL-C, VLDL, ApoB | Increases HDL-C | Injection site reactions, thrombocytopenia (monitor platelets), ↑ LFTs (80 mg dose), arthralgia; high cost — currently restricted to FCS in the U.S. |
| Niacin ⚠️ No longer routinely recommended | 15–25% | 5–10% reduction | 5–10% increase | Flushing (treat with aspirin 30 min before), worsening glycemic control / new-onset T2DM, ↑ LFTs, hyperuricemia |
Mechanism: Apolipoprotein C-III (APOC3) inhibits lipoprotein lipase (LPL), slowing TG clearance. APOC3 inhibitors block hepatic APOC3 production → increased LPL-mediated TG clearance.
Familial Chylomicronemia Syndrome (FCS): A rare genetic condition (biallelic loss-of-function in LPL or LPL-regulating genes) presenting with TG > 1000–2000 mg/dL, recurrent pancreatitis, and poor response to standard TG-lowering therapy. Suspect FCS in patients with severe refractory hypertriglyceridemia and family history of pancreatitis.
- Olezarsen (Tryngolza): Antisense oligonucleotide, 80 mg SQ monthly. Used as adjunct therapy in FCS to lower TG and reduce pancreatitis risk
- Plozasiran: siRNA targeting APOC3, given quarterly, with marked TG lowering in FCS
- Volanesorsen: Approved in Europe/UK/Brazil for FCS — NOT approved in the U.S. due to severe thrombocytopenia risk
- For patients with high ASCVD risk and TG > 150 mg/dL despite lifestyle modification and statin therapy, icosapent ethyl (EPA-only) is the preferred omega-3 agent
- REDUCE-IT trial: Icosapent ethyl 4 g/day reduced major cardiovascular events by 25% in high-risk statin-treated patients
- Icosapent ethyl contains EPA only (no DHA). DHA-containing preparations (Lovaza) may increase LDL-C and are acceptable for patients without high ASCVD risk
- Exception: In patients with paroxysmal atrial fibrillation, prefer fibrates over omega-3s due to AF risk
- Omega-3s should be avoided in TG > 880 mg/dL (chylomicronemia) where strict fat restriction is required
Monitoring TG Therapy
- Severe hypertriglyceridemia (TG > 1000 mg/dL) on strict dietary fat restriction (< 5% fat/day): check TG every 3 days to guide drug initiation
- Moderate or moderate-to-severe hypertriglyceridemia: check TG 6 to 8 weeks after starting or changing drug therapy
High, Moderate, and Low-Intensity Statin Therapy (2026)
| HIGH INTENSITY | MODERATE INTENSITY | LOW INTENSITY |
| Daily dosage lowers LDL-C by approximately ≥ 50% | Daily dosage lowers LDL-C by approximately 30% to 49% | Daily dosage lowers LDL-C by < 30% |
| Atorvastatin (Lipitor) 40–80 mg | Atorvastatin 10–20 mg | Simvastatin 10 mg |
| Rosuvastatin (Crestor) 20–40 mg | Rosuvastatin 5–10 mg | Pravastatin 10–20 mg |
| Simvastatin (Zocor) 20–40 mg | Lovastatin 20 mg | |
| Pravastatin (Pravachol) 40–80 mg | Pitavastatin 1 mg | |
| Lovastatin (Mevacor) 40 mg | ||
| Fluvastatin XL (Lescol XL) 80 mg | ||
| Fluvastatin 40 mg twice daily | ||
| Pitavastatin (Livalo) 2–4 mg |