
Patient will present as → a 48-year-old male presents with two months of worsening shortness of breath, fatigue, and ankle swelling, noting dyspnea on exertion and paroxysmal nocturnal dyspnea. He has a history of heavy alcohol use and recent atrial fibrillation (AF). Exam shows mild resting dyspnea, jugular venous distension, bibasilar crackles, S3 gallop (heard below), displaced PMI, and bilateral edema. Echocardiogram reveals a dilated left ventricle, ejection fraction (EF) 25%, and global hypokinesis. ECG shows AF (controlled rate) and nonspecific ST-T changes. Labs indicate elevated BNP and mild hyponatremia. Chest X-ray shows cardiomegaly and pulmonary congestion. The patient is diagnosed with alcohol-induced DCM, causing HFrEF and AF. Management includes guideline-directed medical therapy (GDMT): sacubitril/valsartan (ARNI) to reduce mortality, carvedilol (beta-blocker) to improve EF, spironolactone (MRA) for EF ≤35%, dapagliflozin (SGLT2i) to lower HF risk, and furosemide for edema. Apixaban is started for AF (CHA2DS2-VASc ≥2). He is counseled on alcohol cessation, low-sodium diet (<2 g/day), and daily weight monitoring. Cardiac rehabilitation is advised. An ICD is considered if EF ≤35% after 3 months of GDMT. Follow-up is scheduled biweekly to titrate GDMT and monitor symptoms, renal function, and potassium. LVAD or transplant is an option for refractory HF.
Dilated Cardiomyopathy (DCM) is a disorder of ventricular dilation and systolic dysfunction, leading to reduced ejection fraction (<40%) and heart failure
- The most common form of cardiomyopathy (approx. 90% of cases)
- Causes include idiopathic (approx. 50%), viral myocarditis (most commonly Coxsackie B; also HIV, Chagas disease), alcohol, chemotherapy (Doxorubicin/Adriamycin), genetic mutations, thyroid diseaseand peripartum cardiomyopathy
- Presents with dyspnea, fatigue, orthopnea, and peripheral edema
- S3 gallop, JVD, and pulmonary crackles, pitting edema
- Displaced PMI (laterally and downward).
- Leads to functional mitral regurgitation due to ventricular dilation
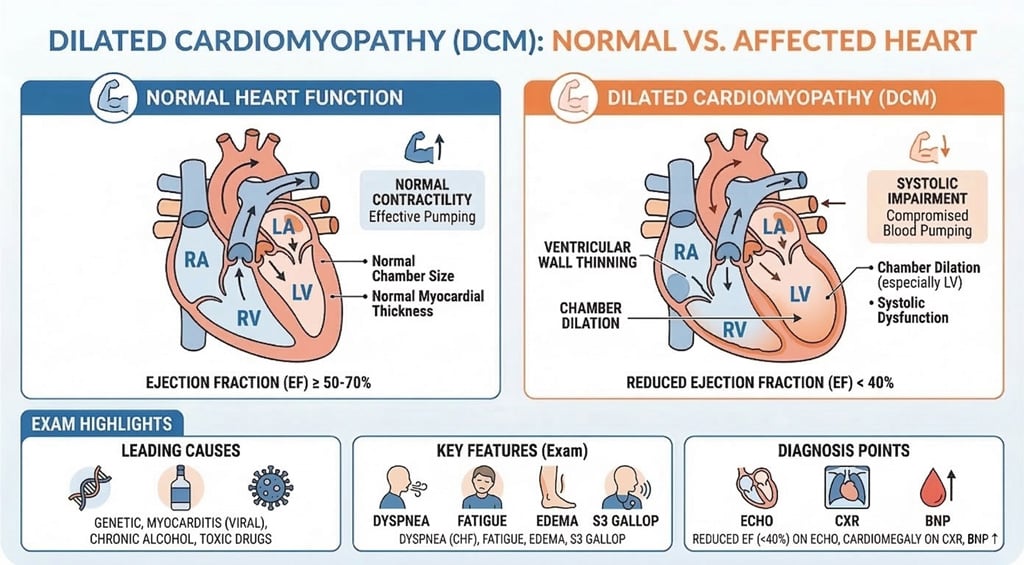
Echocardiography: Gold standard. Shows LV dilation, EF <40% (often <30%), systolic dysfunction
- EKG will show nonspecific ST-T changes, LBBB, or arrhythmias (Afib/VT)
- CXR often shows cardiomegaly (balloon heart), pulmonary congestion/Kerley B lines
- Physical Exam: HF signs—edema, rales, elevated jugular venous pressure (JVP), cardiomegaly (displaced apical impulse), S3 gallop, hepatomegaly
- Additional Tests: BNP/NT-proBNP for HF severity, cardiac MRI for etiology, genetic testing for suspected familial DCM

Dilated cardiomyopathy on CXR
Mnemonic: BAMD (Beta-blockers, ARNI/ACEi/ARB, MRAs, Diuretics/SGLT2i)
- Guideline-Directed Medical Therapy (GDMT):
- ARNI/ACE/ARB: Entresto (sacubitril/valsartan) preferred; otherwise lisinopril/losartan
- Beta-blockers (e.g., carvedilol, metoprolol succinate): Improve EF, survival
- MRAs (e.g., spironolactone or eplerenone): Reduces fibrosis, mortality (for EF ≤35% or symptomatic HF)
- SGLT2i (e.g., dapagliflozin or empagliflozin): Reduces HF hospitalizations and mortality in all HFrEF patients
- Loop diuretics (e.g., furosemide): For fluid overload (edema, dyspnea) only
- Devices:
- Implantable cardioverter-defibrillator (ICD): For EF ≤35%, high arrhythmia risk
- Cardiac resynchronization therapy (CRT): For EF ≤35%, QRS >130 ms, left bundle branch block
- Advanced: Left ventricular assist device (LVAD) or heart transplant for end-stage HF
- Lifestyle: Abstain from alcohol, illicit drugs; manage hypertension, other risk factors
- Note: Digoxin for select cases (e.g., rate control in atrial fibrillation); avoid calcium channel blockers in HFrEF
 Osmosis Osmosis |
|
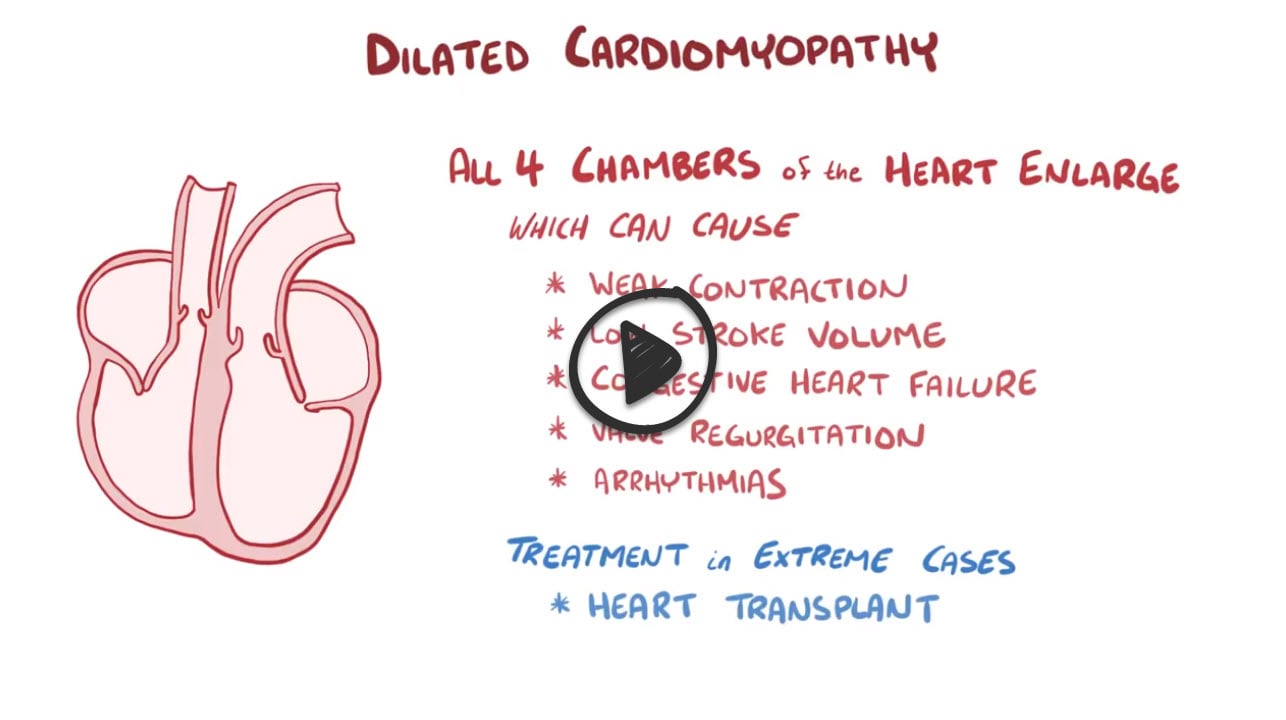 |
Dilated cardiomyopathy is a disease of the heart in which the heart becomes weakened and enlarged, and is unable to pump blood efficiently throughout the body. Therefore, it is commonly described as a contractile or systolic dysfunction. This is the most common form of cardiomyopathy not due to ischemic causes. Although many cases are idiopathic, it is thought that dilated cardiomyopathy is related to damage of the myocardium produced by toxic, metabolic, or infectious agents. Common causes of dilated cardiomyopathy include chronic alcohol abuse, wet beriberi related to thiamine deficiency, coxsackie B infection, cocaine use, Chagas disease, doxorubicin toxicity, hemochromatosis and peripartum cardiomyopathy. On physical exam, an S3 heart sound can be appreciated, due to turbulent blood flow between the walls of the ventricles, as blood flows from the atria in the volume overloaded heart. Dilated cardiomyopathy is also characterized by eccentric hypertrophy in which cardiac sarcomeres are added in series as opposed to parallel.
Play Video + QuizPicmonic Loop diuretics

Loop diuretics are a class of diuretics that inhibit the Na-K-2Cl symporter in the thick ascending limb of the loop of Henle. Furosemide is the generic name for one of the most commonly used loop diuretics and is also known by the trade name, Lasix. These drugs are sulfa drugs, as they contain a sulfonamide group and can cause allergic reactions in patients with sulfa allergies. Loop diuretics often also lead to electrolyte abnormalities, such as hypokalemia and hypocalcemia. Additionally, these drugs can reduce urate excretion, leading to hyperuricemia, and subsequently gout. Ototoxicity is also a serious, but rare adverse effect of loop diuretics.
Play Video + QuizPicmonic Selective β1 blockers

Selective β1 blockers are drugs that act to block β1 adrenergic receptors and typically treat cardiovascular diseases. They work to block the actions of norepinephrine and epinephrine on cardiovascular contractility, chronotropy, and the body’s release of renin. These drugs can be remembered by having the “olol” suffix in their names, such as atenolol, esmolol, and metoprolol. Some β1 blocking drugs also work as partial β agonists at high doses, such as acebutolol.
Play Video + QuizPicmonic Nonselective β-blockers

Nonselective β-blockers were the first generation β-blockers and have antagonistic effects at both β1 (heart, kidney) and β2 receptors (lung, peripheral blood vessels and skeletal muscle) thus preventing direct sympathomimetics such as norepinephrine and epinephrine from binding to these receptors.
Play Video + QuizPicmonic ACE inhibitors

ACE inhibitors are antihypertensive drugs that work by inhibiting the renin-angiotensin-aldosterone-system. They help to lower blood pressure by inhibiting angiotensin converting enzyme and decreasing the amount of angiotensin II and aldosterone. Effects of inhibiting this conversion are translated into lowered arteriolar resistance, and increased venous capacity. This drug class decrease cardiac output and index, and stroke volume. Furthermore, natriuresis is increased, while there is decreased resistance in the blood vessels of the kidney. A side effect of these drugs is increased bradykinin, which may display as a persistant dry cough in patients.
Play Video + QuizQuestion 1 |
enlargement and dilation of all four chambers | |
enlargement and dilation of the left ventricle | |
enlargement and dilation of the right ventricle | |
enlargement and dilation of the right atrium |
Question 2 |
HTN | |
chronic alcoholism | |
viral myocarditis Hint: Viral myocarditis is the second most common cause of non-ischemic cardiomyopathies in the US. (#1 in other parts of the world) | |
genetic predisposition |
Question 3 |
Hypertrophic cardiomyopathy Hint: Hypertrophic cardiomyopathy is characterized by a hyperdynamic left ventricle with asymmetric left ventricular hypertrophy. | |
Dilated cardiomyopathy | |
Restrictive cardiomyopathy Hint: Restrictive cardiomyopathy is characterized more commonly by right-sided heart failure than by left-sided heart failure. There is rapid early filling with diastolic dysfunction. Patients with restrictive cardiomyopathy will have a small thickened left ventricle and a normal or near normal ejection fraction on echocardiogram. | |
Takotsubo cardiomyopathy Hint: Takotsubo cardiomyopathy (broken heart syndrome) is characterized by signs and symptoms of acute coronary syndrome, ST segment elevation on ECG and left ventricular apical dyskinesia. |
|
List |
References: Merck Manual · UpToDate
