| Impaired Systolic Function |
| Dilated Cardiomyopathy |
Patient will present as → a 68-year-old patient who comes to the office because of increased shortness of breath for four months. His symptoms are particularly bad at night. Medical history includes long-standing hypertension and alcoholism. Examination shows a displaced apex beat and normal breath sounds. Cardiac auscultation shows an S3 gallop and a pansystolic murmur radiating to the axilla. The chest X-ray shows an enlarged left ventricular shadow. 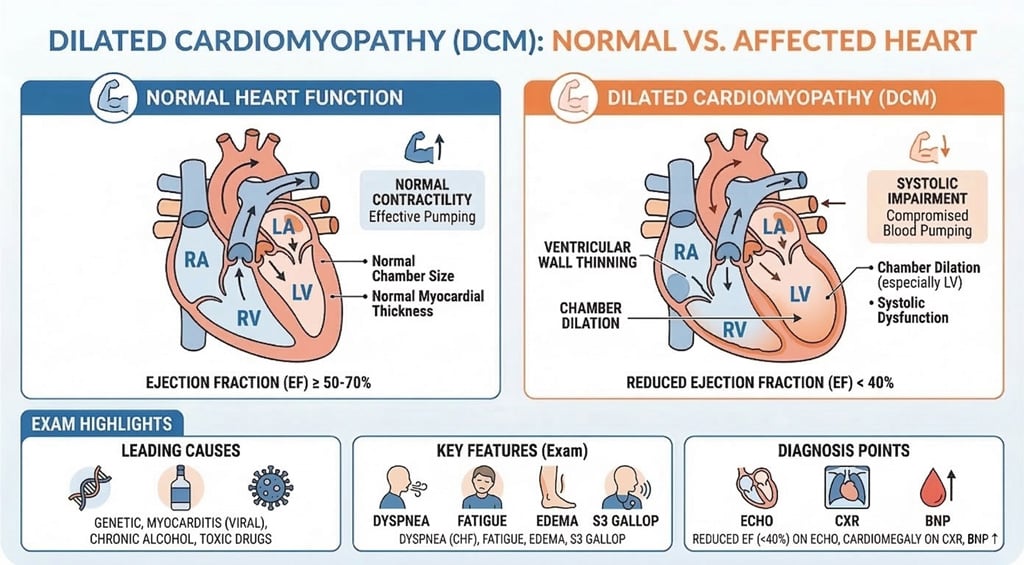
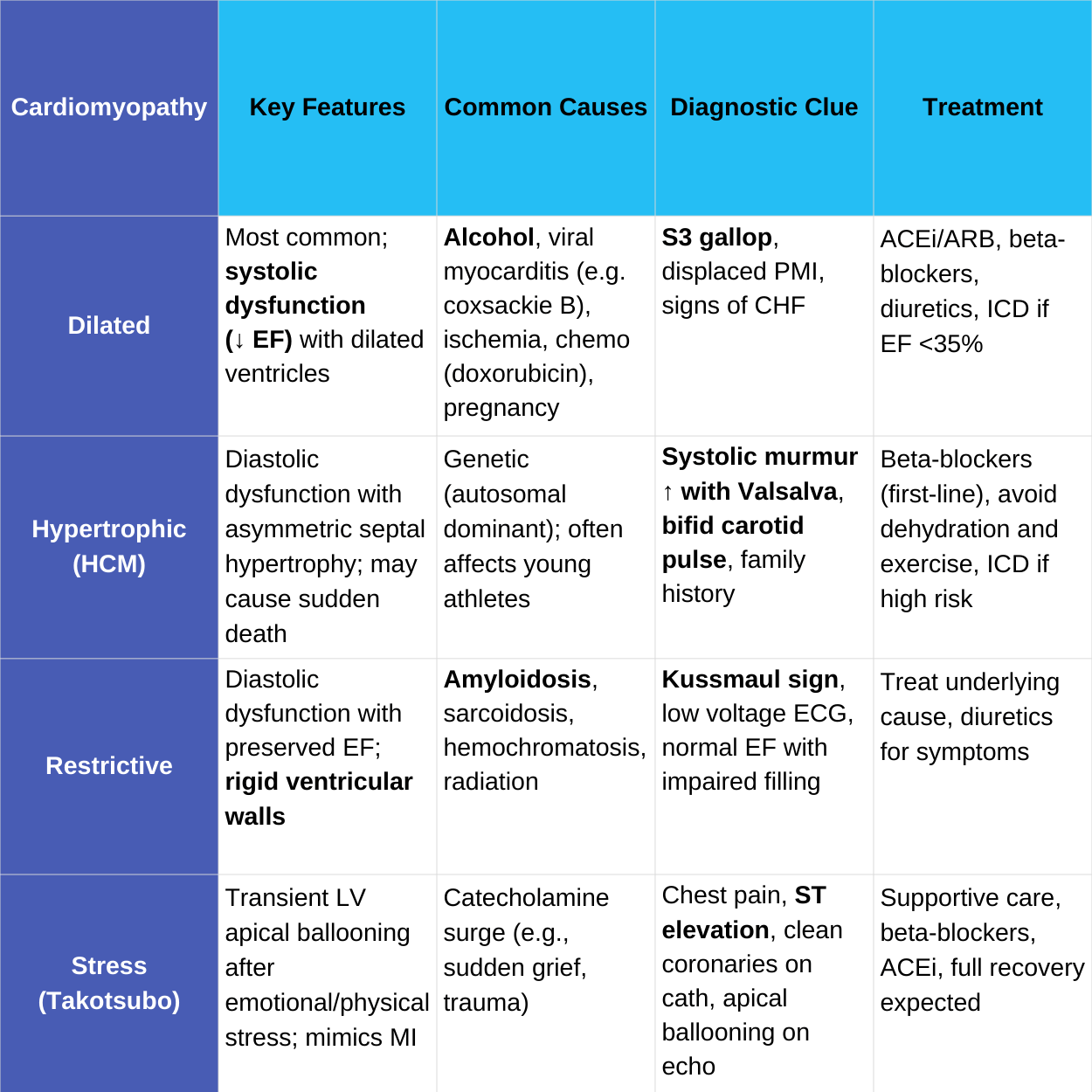
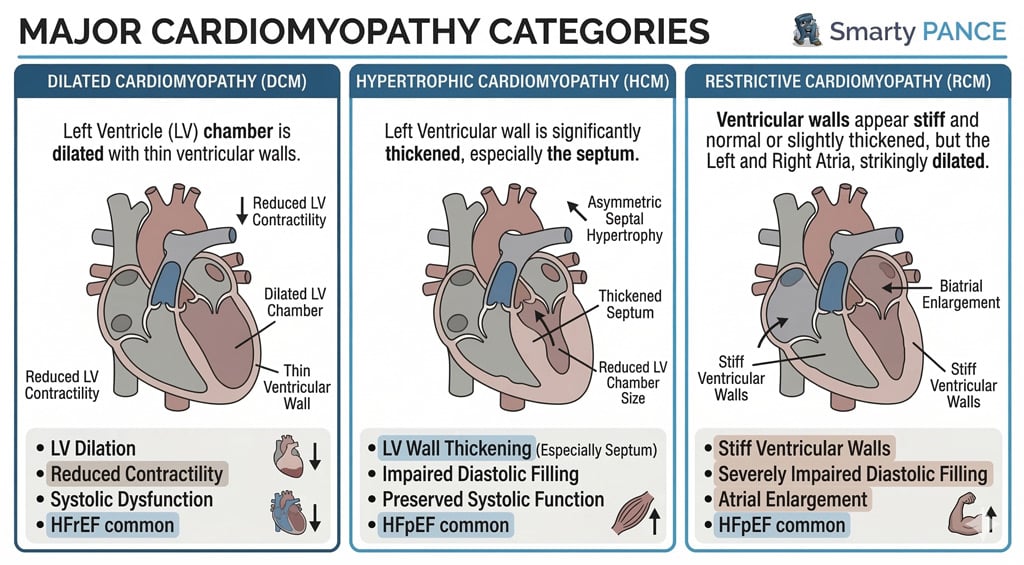
Dilated cardiomyopathy is the most common cardiomyopathy (~90%), with left ventricular (LV) dilation and systolic dysfunction (EF <40%)
- It is a condition in which an index event or process (such as an MI) damages the myocardium, weakening the heart muscle, resulting in reduced strength of ventricular contraction, and dilation of the left ventricle
- Reduced contraction strength, large heart
- Causes include ischemia (CAD, MI, arrhythmia), genetics, excess alcohol, postpartum, chemotherapy, endocrine disorders, viral infections, cocaine use, heavy metals
- Inherited in 1/3 of cases
- Diabetes Link: Hyperglycemia contributes to DCM
- Physical exam: Dyspnea, S3 gallop, rales, cardiomegaly (displaced apical impulse), edema, jugular venous distention - systolic heart failure
- It can cause valve regurgitation and arrhythmias
"An S3 gallop signifies the end of rapid ventricular filling in the setting of fluid overload and is often associated with dilated cardiomyopathy."
DX: Echocardiography is the most definitive diagnosis - demonstrates left ventricular dilation and systolic dysfunction, and low cardiac output with poor EF (<40%)
- EKG will show nonspecific ST/T wave changes, arrhythmias
- CXR often shows a balloon-like heart - will show cardiomegaly and pulmonary congestion
- Other: BNP, cardiac MRI, genetic testing (if familial)
TX: The "Four Pillars" of GDMT (Survival benefit):
-
- 1. ARNI (sacubitril/valsartan) preferred, or ACEi/ARB
- 2. Beta-blockers (Bisoprolol, Carvedilol, Metoprolol Succinate)
- 3. MRAs (e.g., spironolactone): Reduce fibrosis, mortality
- 4. SGLT2i (e.g., dapagliflozin): Standard for all HFrEF patients regardless of diabetes status
- Symptom Management: Loop diuretics (e.g., Furosemide) for fluid overload only (no mortality benefit)
- Devices: ICD (EF ≤35%), CRT (QRS >130 ms)
- Advanced: LVAD, heart transplant
- Lifestyle: No alcohol/drugs, control diabetes
Start sequentially (e.g., ARNI + beta-blocker first, then MRA, SGLT2i)
-
- Adjust for renal function, blood pressure, potassium, or diabetes complications
- Loop diuretics are symptom-driven, not universal
|
| Impaired Diastolic Function |
| Hypertrophic Obstructive Cardiomyopathy (HOCM) |
Patient will present as → a 25-year-old man is brought to the ED because he collapsed while playing tennis 20 minutes ago. Medical history includes unexplained chest pain and shortness of breath while exercising for three years. Family history includes an uncle who died of an unknown cardiac pathology at the age of 23. Cardiac auscultation shows a 2/6 systolic murmur is heard at the left of the sternum between the first two ribs. The murmur becomes louder when the patient performs a Valsalva maneuver and decreases with squatting. 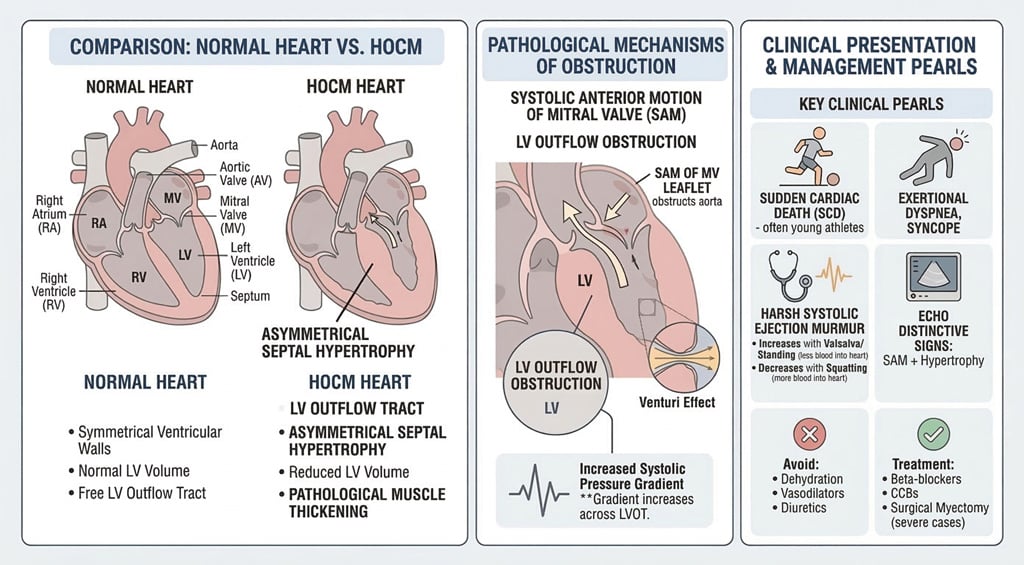
The hypertrophic portion of the septum - LV outflow tract is narrowed during systole, and obstruction worsens with increased contractility
Presentation: A young athlete with a positive family history has a sudden death or syncopal episode
- Inherited autosomal dominant - screen family members
- Presents in early adulthood
- Not to be confused with hypertrophy of an elite athlete
Physical Exam:
- Sustained PMI, bifid pulse, S4 gallop
- Murmur: High-pitched mid-systolic murmur at LLSB. Increased with Valsalva and standing (less blood in the chamber)
- Decreased with squatting (more blood in the chamber)
"The murmur due to HCM will increase in intensity with any maneuver that decreases the volume of blood in the left ventricle (such as standing abruptly or the strain phase of a Valsalva maneuver ). "
DX: Diagnosis is by echocardiography or MRI
- Echo is the key to diagnosis and will show left ventricular hypertrophy with a thickened septum, a small left ventricle, and diastolic dysfunction
- EKG will show nonspecific ST and T-wave changes and left ventricular hypertrophy
TX:
- First-line: nonvasodilating beta-blockers (e.g., metoprolol) to reduce contractility, slow heart rate, and improve diastolic filling
- If beta-blockers are not tolerated or ineffective: non-dihydropyridine calcium channel blockers such as verapamil or diltiazem
- Cardiac myosin inhibitor: mavacamten may be used for symptomatic obstructive HCM under cardiology supervision
- Avoid nitrates, aggressive diuresis, and vasodilators in symptomatic obstructive HCM because reduced preload/afterload can worsen LV outflow tract obstruction
- Digoxin is contraindicated in obstructive HCM because increased contractility can worsen obstruction
- ICD: consider for patients at increased sudden cardiac death risk, including prior cardiac arrest, sustained ventricular tachycardia, unexplained syncope, massive LVH, apical aneurysm, reduced EF, or strong family history
- Septal reduction therapy: surgical myectomy or alcohol septal ablation if symptoms persist despite optimal medical therapy
|
| Restrictive Cardiomyopathy |
Patient will present as → a 58-year-old man complaining of several months of worsening shortness of breath and ankle swelling. He denies palpitations, lightheadedness, syncope, or chest pain. He has a past medical history significant for hereditary hemochromatosis. On physical exam, his temperature is 37°C (98.6°F), pulse is 78, blood pressure is 130/72 mm Hg, and respiratory rate is 16. He has elevated jugular venous pressure, diminished breath sounds at the lung bases, tender hepatomegaly, and bilateral pitting ankle edema. There are no murmurs, rubs, or gallops. EKG shows low-voltage QRS complexes without any signs of ischemia. His chest x-ray shows a normal-sized heart and bilateral pleural effusions. Echocardiography shows symmetrical thickening of the left ventricle, normal left ventricular volume, and mildly reduced systolic function. 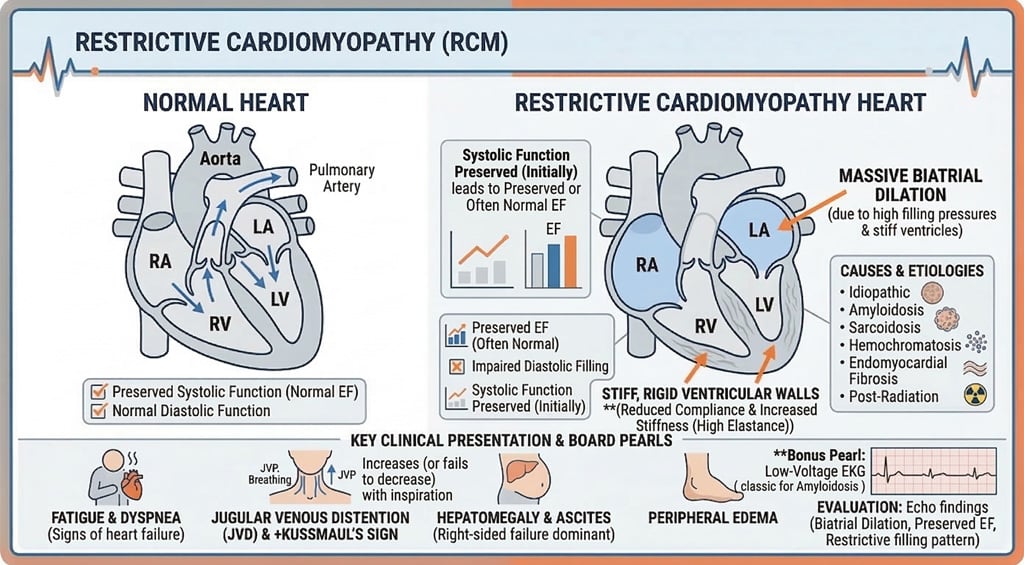
Right heart failure with a history of an infiltrative process
RCM is a filling problem (diastolic), not a pumping problem (systolic). It’s "stiff," whereas Hypertrophic Cardiomyopathy (HCM) is "thick" and often obstructive.
- Etiology: Amyloidosis (ATTR or AL), sarcoidosis, hemochromatosis, scleroderma, fibrosis, and cancer (radiation and chemotherapy)
- Physical Exam:
- Pulmonary HTN present
- Normal ejection fraction, normal heart size, large atria, normal left ventricular wall, early diastolic filling
- Hepatomegaly and ascites
- Peripheral edema
DX: Echocardiography typically shows biatrial enlargement, nondilated ventricles, preserved or mildly reduced EF, and abnormal diastolic filling
- ECG is often nonspecifically abnormal and may show low voltage, especially with amyloidosis
- Cardiac MRI can help identify infiltrative myocardial disease
- Cardiac catheterization may show restrictive filling physiology
- Myocardial biopsy can confirm infiltrative disease when noninvasive testing is inconclusive
- CXR: pulmonary vascular congestion or pleural effusions with a normal-sized heart
TX: Treat the underlying cause
- ATTR cardiac amyloidosis: tafamidis
- AL amyloidosis: hematology-directed plasma cell therapy and urgent specialty referral
- Sarcoidosis: corticosteroids or other immunosuppressive therapy when clinically indicated
- Diuretics may help congestion but must be used cautiously because these patients are preload dependent
|
| Stress cardiomyopathy |
Patient will present as → a 62-year-old female arrives with sudden chest pain and shortness of breath after receiving distressing news. She has hypertension, is postmenopausal, and appears anxious but hemodynamically stable. ECG shows anterior ST elevations, and troponin is mildly elevated but out of proportion to the ECG findings. Coronary angiography reveals no significant stenosis. An echocardiogram demonstrates apical ballooning with preserved basal function, confirming stress cardiomyopathy, a transient left ventricular dysfunction due to intense emotional stress. She is started on beta-blockers and an ACE inhibitor to support myocardial recovery. Anticoagulation is considered if an apical thrombus is detected. The patient is counseled that the prognosis is excellent with appropriate treatment, and a repeat echocardiogram is planned in 4-6 weeks to confirm resolution. 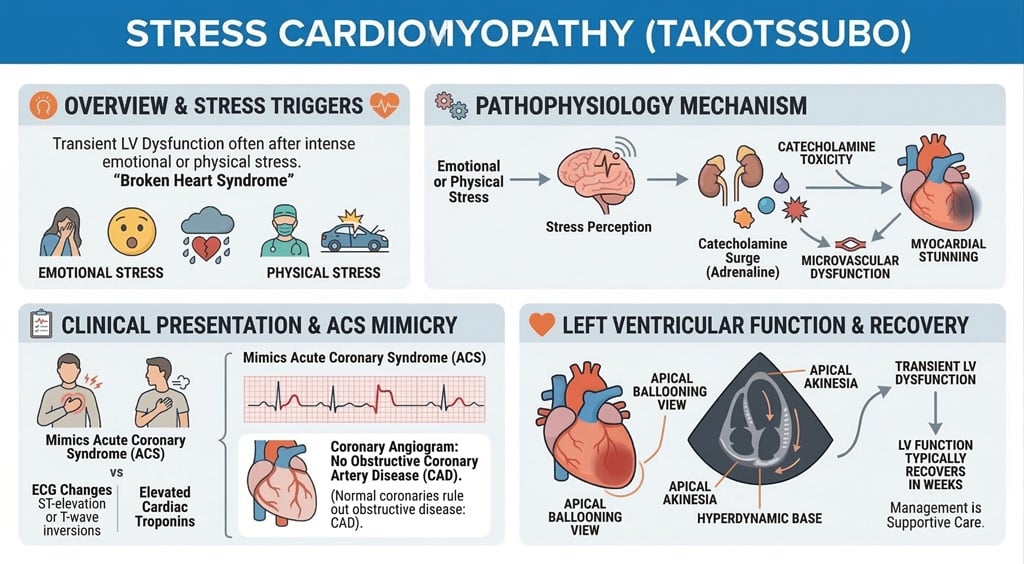
Stress Cardiomyopathy (Takotsubo Syndrome) is a transient, stress-induced cardiomyopathy characterized by sudden, reversible left ventricular dysfunction, often mimicking acute coronary syndrome (ACS)
- It primarily affects postmenopausal women, accounting for over 90% of cases
- Common triggers include emotional or physical stress, such as grief ("broken heart syndrome"), surgery, or severe illness
- Symptoms are indistinguishable from acute myocardial infarction -> acute chest pain, dyspnea, and sometimes syncope
- Thought to result from catecholamine surge leading to myocardial stunning and microvascular dysfunction
- The key distinguishing feature is absence of obstructive coronary artery disease despite clinical and electrocardiographic features resembling myocardial infarction
DX:
- ECG demonstrates ST-segment elevation (44%) or T-wave inversions, mimicking STEMI
- Troponins are elevated in all patients with stress cardiomyopathy, but disproportionally lower than expected for the degree of ECG changes
- Echocardiography demonstrates apical ballooning (dyskinetic apex with hyperkinetic basal segments) or other patterns of regional wall motion abnormality not corresponding to a single coronary artery territory
- Coronary angiography demonstrates normal coronary arteries (a key distinguishing feature from ACS)
- Brain natriuretic peptide (BNP) levels may be elevated, which often peak later than troponin levels
TX:
- Supportive care with beta-blockers, ACE inhibitors, and anticoagulation if apical thrombus
- Avoid inotropes in severe cases due to risk of worsening outflow obstruction; IV fluids and vasopressors may be used for hypotension
- Treat stressors and provide emotional and physical support
- The prognosis is excellent, with recovery in 1-4 weeks; complications include heart failure, arrhythmias, or rarely cardiogenic shock. Recurrence is rare
|

{kind=link}