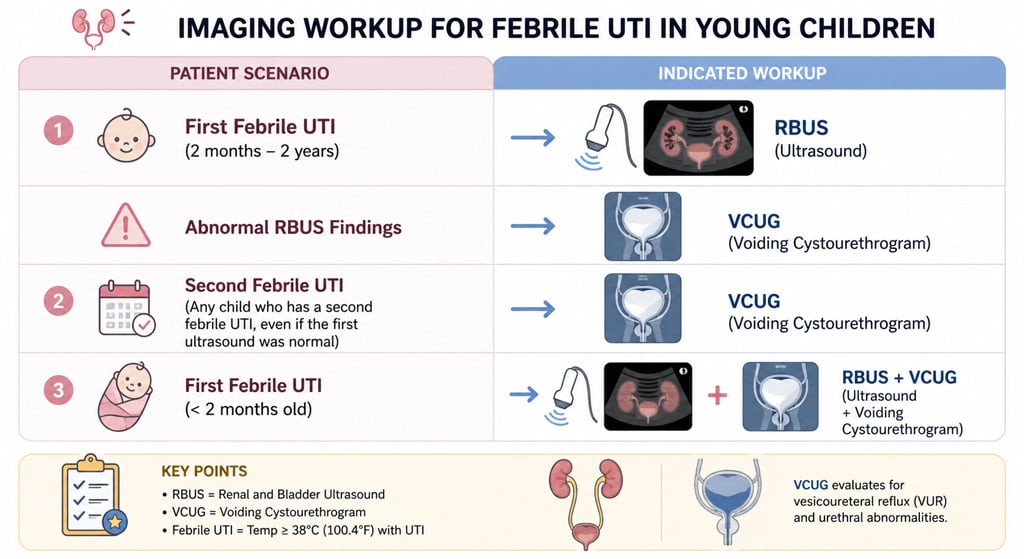
Patient will present as → a 1-year-old girl presents with a temperature of 103.1°F and irritability. This is her second febrile UTI in the last six months. Urine culture reveals >100,000 CFU/mL of E. coli. She is treated with a 10-day course of Cefdinir. Once the infection is cleared, a renal and bladder ultrasound (RBUS) is performed, and is normal. Due to the recurrent nature of her infections, a voiding cystourethrogram (VCUG) is performed, which reveals bilateral Grade III vesicoureteral reflux.
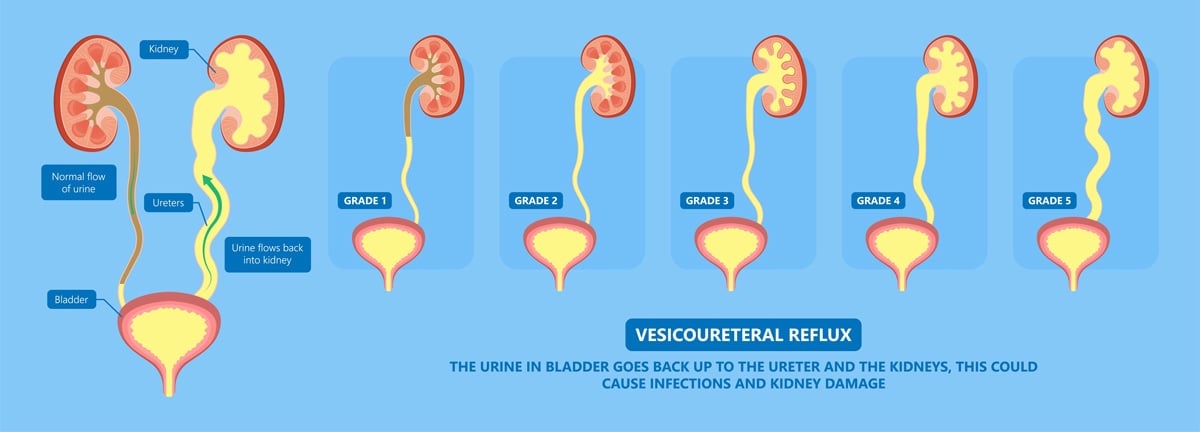
Vesicoureteral reflux (VUR) is a condition in which urine flows retrograde, or backward, from the bladder into the ureters/kidneys
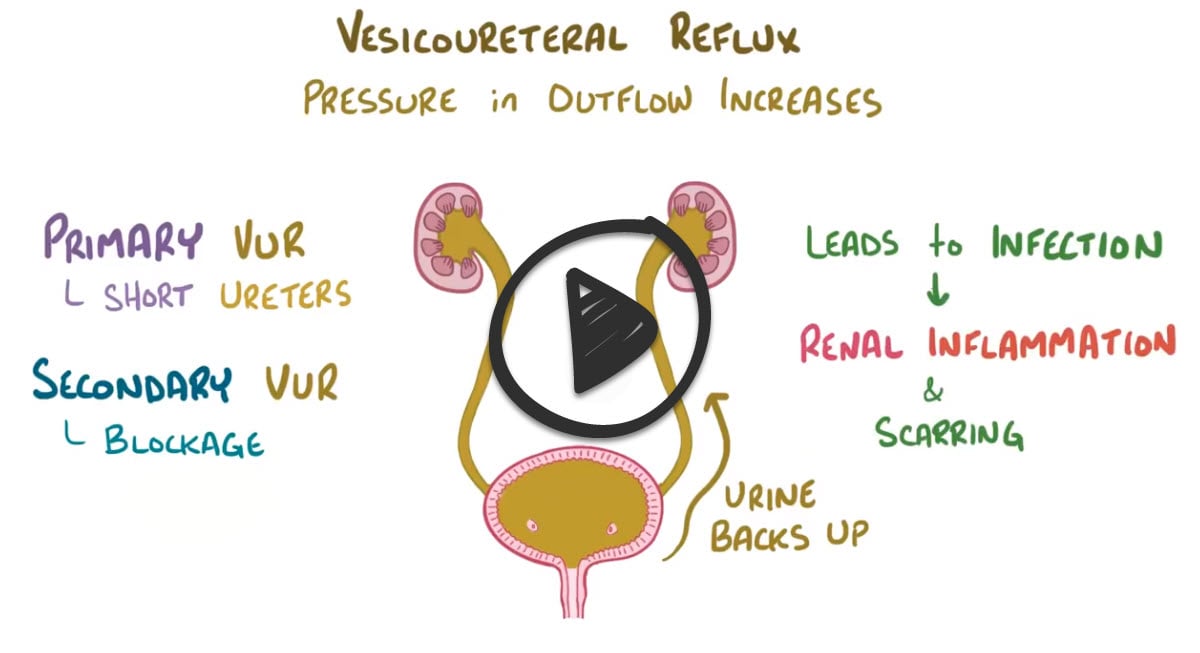
There are two types of vesicoureteral reflux
- Primary vesicoureteral reflux is the most common type and happens when a child is born with a defect at the ureterovesical junction
- In secondary vesicoureteral reflux, there’s an obstruction at some point in the urinary tract that causes an increase in pressure, causing urine to flow backward into the ureters or kidneys
- Secondary vesicoureteral reflux is most commonly caused by recurrent urinary tract infections
- Other causes include posterior urethral valve disorder, and neurogenic bladder
- In young female patients, any history that points to recurrent infection, especially cystitis or pyelonephritis, should trigger an evaluation for vesicoureteral reflux (VUR)
© Pepermpron / Adobe Stock
Renal ultrasound: evaluate for hydronephrosis and renal size/scarring (DMSA scan for scarring)
- Voiding cystourethrogram (VCUG) — gold standard: demonstrates reflux grade and anatomy during voiding
- Monitor by using serial ultrasonography and VCUGs
{kind=link}
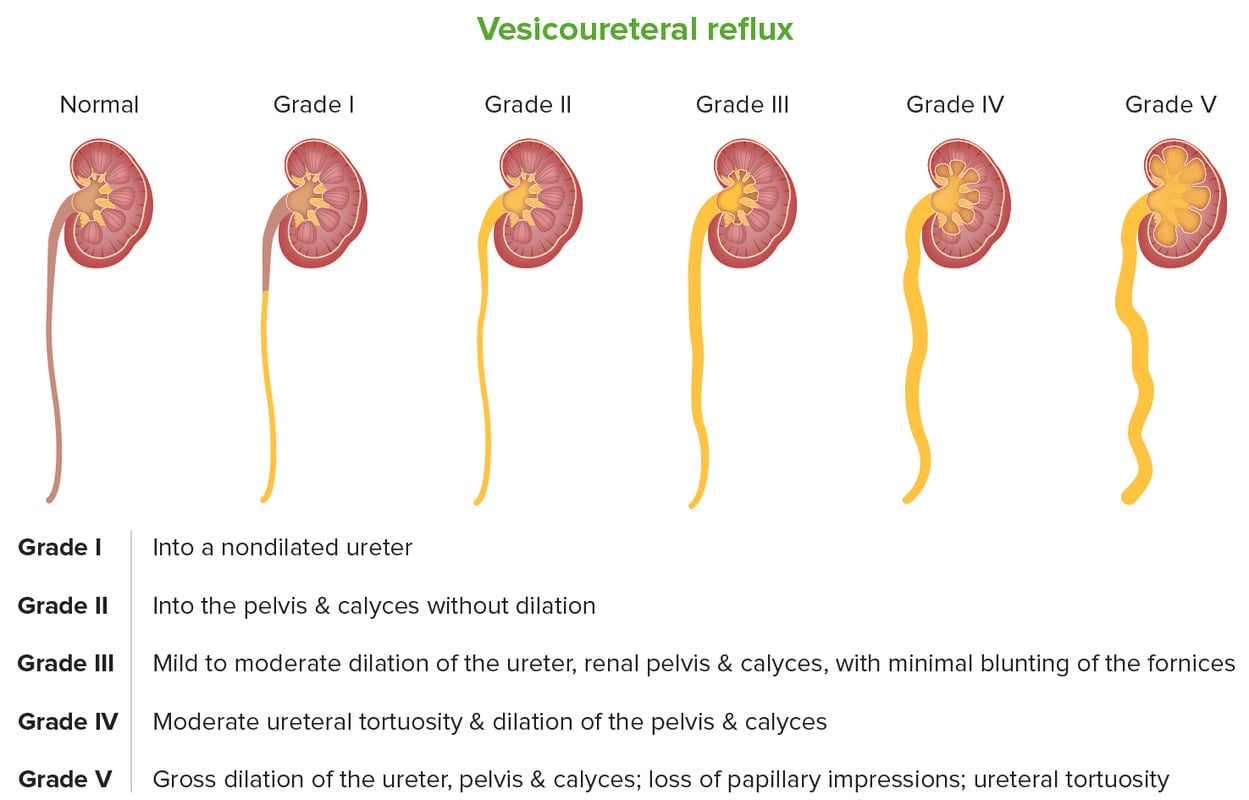
- Grade I – reflux into non-dilated ureter
- Grade II – reflux into the renal pelvis and calyces without dilatation
- Grade III – mild/moderate dilatation of the ureter, renal pelvis, and calyces with minimal blunting of the fornices
- Grade IV – dilation of the renal pelvis and calyces with moderate ureteral tortuosity
- Grade V – gross dilatation of the ureter, pelvis, and calyces; ureteral tortuosity; loss of papillary impressions
Mild to moderate VUR often resolves spontaneously, but the more serious disease may require surgical intervention
- Children with newly diagnosed VUR are given prophylactic antibiotics depending on their clinical course
- Antibiotics are administered nightly at half the normal therapeutic dose
 Osmosis Osmosis |
|
 |
Question 1 |
Dark-colored urine Hint: Dark-colored urine and painless hematuria are concerning history findings, but point more toward a renal cause of disease. | |
Epigastric abdominal pain Hint: Epigastric abdominal pain is not seen in patients with VUR and any pain associated with VUR, if present, would most likely be located in the renal or suprapubic areas. | |
Nocturnal enuresis Hint: Although incontinence can be a sign of cystitis, enuresis limited to night would likely not be present in the presence of infection. | |
Painless hematuria Hint: Dark-colored urine and painless hematuria are concerning history findings, but point more toward a renal cause of disease. | |
Recurrent cystitis |
Question 2 |
Continue current antibiotic prophylaxis regimen Hint: Continuing the ineffective antibiotic prophylaxis would not address the breakthrough infection or high-grade reflux. | |
Obtain DMSA (dimercapto succinic acid) renal scan Hint: A DMSA renal scan could evaluate for new scarring but does not address definitive correction of reflux. | |
Start cephalexin for UTI treatment Hint: Cephalexin would treat the acute UTI but does not correct the underlying reflux. | |
Consider surgical correction | |
Stop antibiotic prophylaxis Hint: Stopping antibiotic prophylaxis is not appropriate given his high-grade reflux and recurrent infections. |
|
List |
References: Merck Manual · UpToDate