The NCCPA™ PANCE Genitourinary Content Blueprint penile disorders
| Erectile dysfunction | Hypospadias/epispadias | Paraphimosis/phimosis | |
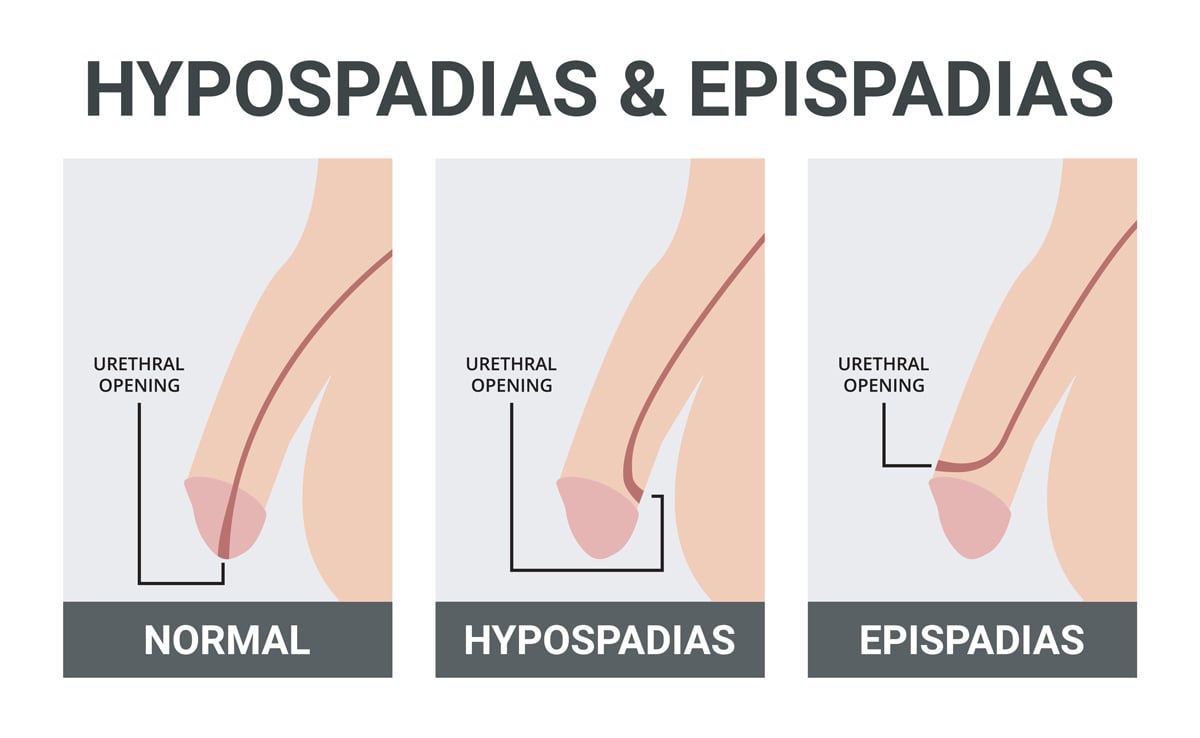
| Description | Inability to achieve or maintain an erection sufficient for sexual intercourse | A birth defect in which the opening of the urethra is not at the tip of the penis | A condition in which the foreskin is retracted behind the glans penis and cannot be pulled back forward |
| Symptoms | Difficulty achieving or maintaining an erection | The urethral opening is not at the tip of the penis
Epispadias is when the urethra opens onto the topside of the penile shaft Hypospadias (more common than epispadias) is when the urethra opens onto the bottom (underside) of the penile shaft |
The foreskin is retracted behind the glans penis and cannot be pulled back forward |
| Causes | Vascular disease, neurological disorders, hormonal imbalances, medications, and psychological factors | Genetics, environmental factors | Recurrent retraction of the foreskin, inflammation of the foreskin, trauma to the penis |
| Treatment | Lifestyle changes, medications, and surgery | Treatment is surgical repair, usually performed before 1-2 years of age | Treat with betamethasone topically. If there is no improvement, circumcision |
Occurs when a man can't get or keep an erection firm enough for sexual intercourse
- Psychological
- Organic causes include hypertension, neurological problems from diabetes, and hormonal dysfunction
- Medication side effects
- Nocturnal penile tumescence used to evaluate sleep erections
- Do not use with nitrates may cause hypotension
DX: Detailed history and examination, including a DRE and neurologic examination. Assess for signs of PAD
- Laboratory tests—Obtain a CBC, chemistry panel, fasting glucose, and lipid profile
- If there is hypogonadism or loss of libido, order serum testosterone, prolactin levels, and thyroid profile
- Nocturnal penile tumescence—If normal erections occur during sleep, a psychogenic cause is likely. If not, the cause is probably organic.
- Vascular testing—Evaluate arterial inflow and venous trapping of blood. Tests include intracavernosal injection of vasoactive substances, duplex ultrasound, and arteriography
- Psychologic testing may be appropriate in some cases
TX: Treat with phosphodiesterase 5 inhibitors Sildenafil (Viagra), Tadalafil (Cialis), Vardenafil (Levitra)
- Weight loss, smoking, and alcohol cessation, hormone replacement and vacuum erection devices, and surgery
© SM 1000 by Adobe Stock
Epispadias is when the urethra opens onto the topside of the penile shaft
- The position of the urethral meatus defines the type of epispadias
- Penopubic - at the base of the penis and abdominal wall come together (most severe)
- Penile - along the shaft of the penis
- Glanular - near the head of the penis (least severe)
DX: Diagnosis is usually made clinically during the newborn exam, but imaging studies (excretory urogram) can aid in the diagnosis
TX: Treatment is surgical repair (urethroplasty), usually between 6 and 12 months of age, with 18 months being the general upper limit for the primary repair
- DO NOT CIRCUMCISE if hypospadias OR epispadias — the foreskin tissue is essential for surgical reconstruction.
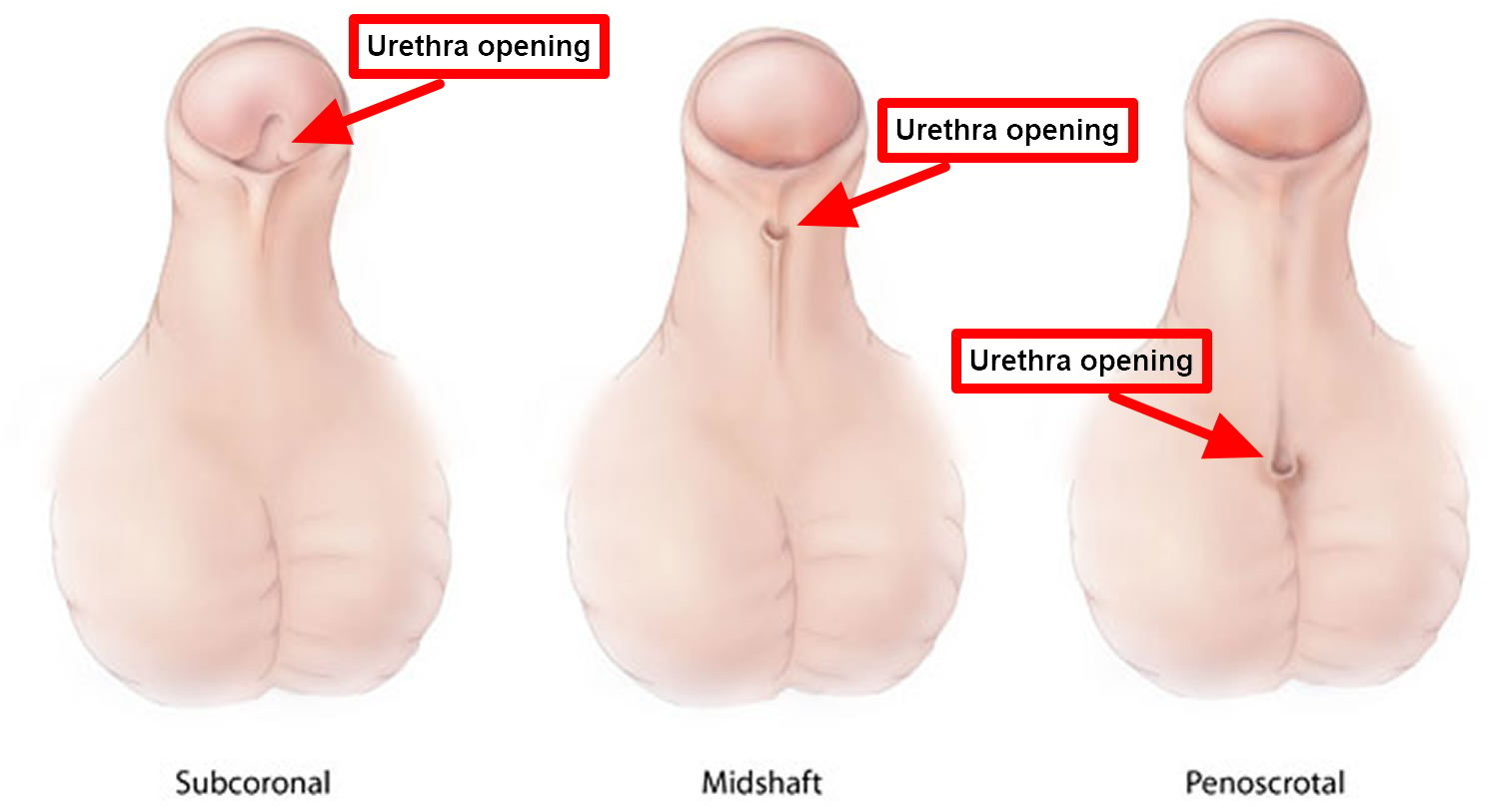
Hypospadias (more common than epispadias) is when the urethra opens onto the ventral (underside) of the penile shaft
- The position of the urethral meatus defines the type of hypospadias
- Glanular - head of the penis (least severe)
- Midshaft - middle of the penis
- Penoscrotal - where the penis and scrotum come together (most severe)
DX: Diagnosis is usually made clinically during the newborn exam, but imaging studies (excretory urogram) can aid in the diagnosis
TX: Treatment is surgical repair (urethroplasty), usually between 6 and 12 months of age, with 18 months being the general upper limit for the primary repair

Hypospadias and two fistulas
ReelDx Virtual Rounds (Paraphimosis)
{kind=link}
{kind=link}
Mnemonic: Paraphimosis = Paramedics (Emergency). Phimosis = Family Practice (Non-emergent)
Paraphimosis is the inability to return the foreskin to its normal position
- Entrapment of the foreskin behind the glans
- It causes a tourniquet effect and is a medical emergency
- More acute than phimosis
DX: The diagnosis of paraphimosis is based on clinical findings
TX: Treat by applying firm circumferential compression to the glans with the hand - may relieve edema sufficiently to allow the foreskin to be restored to its normal position.
- If this technique is ineffective, a dorsal slit using a local anesthetic relieves the condition temporarily
- Circumcision is then done when the edema has resolved

Paraphimosis is the entrapment of the foreskin in the retracted position
Phimosis is the inability to retract the foreskin
- Usually resolves by age five
- Unable to retract the foreskin
- More chronic than paraphimosis
DX: The diagnosis of paraphimosis is based on clinical findings
TX: Treat with betamethasone topically. If there is no improvement → circumcision

Erect phimosis—the foreskin is in the normal position and cannot be retracted
Priapism is a urological emergency that involves a prolonged, often painful erection lasting more than two to four hours, unrelated to sexual stimulation or desire
- Classified into ischemic (low-flow) and non-ischemic (high-flow) types
- Ischemic priapism (most common) involves painful, rigid erection and is a medical emergency
- Non-ischemic priapism involves a less painful, partially rigid erection and is usually related to trauma
- Common causes include sickle cell disease, medications (e.g., PDE-5 inhibitors, antidepressants, antipsychotics), and spinal cord injury
DX: The diagnosis of priapism is made on the basis of visual inspection of the penis, which reveals an erection that has been present for more than two to four hours in the absence of sexual excitation
- Cavernous blood gas analysis and/or Doppler ultrasonography can distinguish between ischemic and non-ischemic priapism
TX:
- Ischemic priapism treatment: Aspiration of corpora cavernosa, intracavernosal injection of phenylephrine, and surgical shunt if refractory
- Non-ischemic priapism treatment: Often conservative management, including ice packs and compression; arterial embolization for persistent cases

Color Doppler ultrasound demonstrating a hypoechoic collection that corresponds to hematoma with arteriovenous fistula secondary to traumatic injury of the penis due to impact with bicycle handlebars, resulting in high-flow priapism.