 Lecture
Lecture
Patient will present as → a 65-year-old man presents to your clinic complaining of frequent urination, especially at night, and a sensation that his bladder is not completely emptying. He also reports a weak urinary stream and occasional dribbling. He has no history of urinary tract infections, hematuria, or renal stones. His medical history is significant for hypertension, for which he takes hydrochlorothiazide. On digital rectal exam, his prostate is uniformly enlarged, firm, and rubbery. Urinalysis is unremarkable, and his serum prostate-specific antigen (PSA) level is 5.

To watch this and all of Joe Gilboy PA-C's video lessons you must be a member. Members can log in here or join now.
BPH is part of the normal aging process but only sometimes causes symptoms (50% of men develop BPH by 60 and > 90% by age 85)
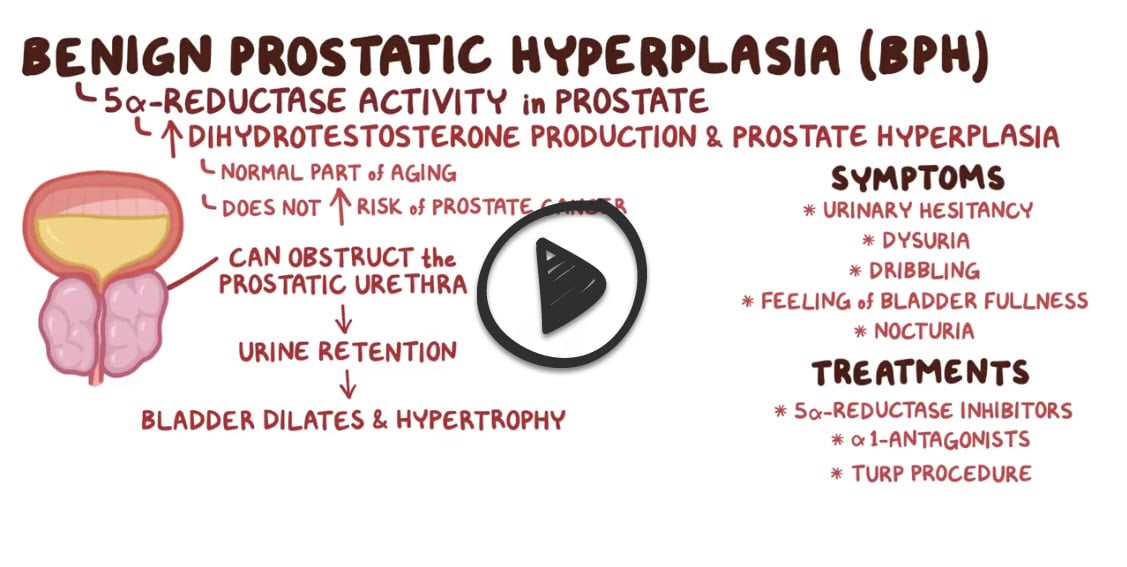
- Caused by hyperplasia of prostatic epithelial, stromal cells → formation of nodules in periurethral (transition) zone → narrowing of urethral canal → urethral compression → obstruction of the urinary outlet
- Features: A decreased force of urinary stream, hesitancy (stop and start) and straining, postvoid dribbling, incomplete emptying, frequency, nocturia, urgency, recurrent UTIs
- Acute urinary retention can develop with exposure to cold, prolonged attempts to postpone voiding, immobilization, or use of anesthetics, anticholinergics, sympathomimetics, opioids, or alcohol
- In men with BPH, avoid use of anticholinergics, sympathomimetics, and opioids
{kind=link}

The panel on the left shows the normal prostate and the flow of urine from the bladder through the urethra. The panel on the right shows an enlarged prostate pressing on the bladder and urethra, blocking the flow of urine.
A digital rectal exam - will demonstrate a uniformly enlarged, firm, and rubbery prostate
- Although cancer may cause a stony, hard, nodular, irregularly enlarged prostate, most patients with cancer, BPH, or both have a benign feeling, enlarged prostate. Thus, testing should be considered for patients with symptoms or palpable prostate abnormalities
PSA is often ↑ in BPH - correlate with risk of symptom progression
- PSA is considered normal < 4
- PSA > 4 think BPH, prostate CA, and prostatitis
Urinalysis is used to rule out other conditions
Observation is reasonable if mild symptoms - patients should be monitored annually
1. Alpha-blockers cause urethral relaxation and rapid symptom relief
- α-1 blockers - tamsulosin (Flomax) most uroselective, provides rapid symptom relief - smooth muscle relaxation of prostate and bladder neck decreases urethral resistance and obstruction, which increases urinary flow and can cause dizziness and orthostatic hypotension as well as retrograde ejaculation
- Doxazosin (Cardura) - Non-selective alpha-1 blocker, used for both BPH and hypertension
2. 5 ∝ reductase inhibitors (5ARI) (REDUCE THE SIZE) shrink an enlarged prostate
- 5-α reductase inhibitors - finasteride and dutasteride (androgen inhibitor - inhibits the conversion of testosterone to dihydrotestosterone, suppressing prostate growth and reducing bladder outlet obstruction). Has a positive effect on the clinical course of BPH
3. Phosphodiesterase type 5 inhibitor (PDE5 inhibitor) - tadalafil, in men with BPH-related symptoms and erectile dysfunction
- PDE5 inhibitors block the PDE5 enzyme to prevent it from working. This inhibition relaxes the blood vessels and increases blood flow
Combination therapy:
- Combination of alpha-adrenergic blockers and 5-alpha reductase inhibitors in men who have demonstrated prostate enlargement and moderate to severe symptoms of BPH
- Combination therapy with PDE5 inhibitors and alpha 1-adrenergic blockers seemed to have an additive beneficial effect on BPH/lower urinary tract symptoms compared with monotherapy
Surgery is done when patients do not respond to drug therapy or develop complications such as recurrent urinary tract infection, urinary calculi, severe bladder dysfunction, or upper tract dilation.
- TURP (transurethral resection of the prostate) - removes excess prostate tissue to relieve obstruction - sexual dysfunction and urinary incontinence
- Transurethral incision of the prostate (TUIP) - electric current to make incisions in prostate - no tissue is removed
- Open prostatectomy - reserved for very large prostates (>80–100 grams) or cases with concomitant bladder pathology (e.g., large bladder stones)
Step 1: Are any of the following present?
PSA ≥ 4 ng/mL, history of prostate cancer, recurrent UTI, bladder stones, gross hematuria, hydronephrosis, refractory urinary retention, progressive kidney dysfunction
→ Yes: Refer to urology
→ No: Proceed to Step 2
Step 2: Initiate lifestyle & behavioral interventions
(e.g., fluid timing, bladder training, reducing alcohol/caffeine)
→ Reassess symptoms
Step 3: Are symptoms minimally bothersome?
→ Yes: Continue non-pharmacologic management only
→ No (moderate to severe): Proceed to Step 4
Step 4: Is the prostate enlarged? (PSA ≥ 1.5 ng/mL, DRE, or imaging >30g)
→ Yes: Start alpha-blocker (eg, tamsulosin 0.4 mg daily) + 5-alpha-reductase inhibitor (5-ARI) (eg, finasteride 5 mg daily)
→ No: Start alpha-blocker monotherapy
→ If erectile dysfunction: Consider PDE-5 inhibitor (eg, tadalafil 5 mg daily)
→ If OAB symptoms predominate: Add beta-3 agonist (eg, mirabegron 25–50 mg daily) or antimuscarinic (eg, oxybutynin 5 mg BID–TID or ER 5–10 mg daily)
Step 5: Are symptoms refractory or worsening?
→ Yes: Refer to urology for further evaluation ± surgical management
→ No: Continue current management and monitor regularly
 Osmosis Osmosis |
|
 |
 BPH is characterized by increased epithelial cells and stromal components of the lateral and middle glands of the prostate. It can lead to compression of the urethra and various urinary manifestations. Accurately diagnosing BPH is extremely important as more serious conditions, such as prostate cancer must be ruled out. Therapy is typically medical; however, in certain instances, more invasive therapy (i.e. TURP) may be needed.
BPH is characterized by increased epithelial cells and stromal components of the lateral and middle glands of the prostate. It can lead to compression of the urethra and various urinary manifestations. Accurately diagnosing BPH is extremely important as more serious conditions, such as prostate cancer must be ruled out. Therapy is typically medical; however, in certain instances, more invasive therapy (i.e. TURP) may be needed.
Question 1 |
benign prostatic hypertrophy (BPH) | |
carcinoma of the bladder | |
prostatic carcinoma | |
urethral stricture | |
chronic prostatitis |
Question 2 |
dysuria | |
daytime frequency | |
incomplete voiding | |
urgency | |
all of the above |
Question 3 |
finasteride | |
prazosin | |
terazosin | |
a, b, and c |
Question 4 |
symptom assessment with a validated screening tool | |
transrectal ultrasound examination | |
computed tomography (CT) scan of the pelvis | |
a and b |
Question 5 |
transurethral resection of the prostate (TURP) | |
open prostatectomy | |
transurethral incision of the prostate | |
hyperthermia of the prostate | |
balloon dilation of the prostate |
|
List |
References: Merck Manual · UpToDate