 Lecture
Lecture


A 53 y/o with weakness, polydipsia, and polyuria
Patient will present as → a 35-year-old Mexican American male complaining of increased thirst, frequent urination, hunger, fatigue, and blurred vision. A random finger stick blood glucose is 225.
Diabetes mellitus medications

To watch this, and all of Joe-Gilboy PA-C's marvelous video lessons you must be a member. Members can login here or join now.
Know Your Medication - Side Effects and Functions
- Metformin (Glucophage, Glumetza, Fortamet, Riomet):
- Mechanism: Reduces hepatic glucose production, increases peripheral glucose uptake (improves insulin sensitivity), and decreases intestinal glucose absorption. These actions contribute to weight neutrality or weight loss and are effective in lowering blood glucose without increasing insulin levels.
- Side Effects: Risk of lactic acidosis, particularly in renal impairment. Requires discontinuation 24 hours before contrast studies and resumption 48 hours after, with monitoring of creatinine. Discontinue if creatinine is >1.5 mg/dL.
- Sulfonylureas - Glyburide (Diabeta, Glynase), Glipizide (Glucotrol, Glucotrol XL), Glimepiride (Amaryl):
- Mechanism: Stimulates insulin release from pancreatic beta cells (insulin secretagogue), increasing insulin levels regardless of glucose levels.
- Side Effects: Significant risk of hypoglycemia and weight gain. Particularly risky in elderly or those with renal impairment.
- Thiazolidinediones - Pioglitazone (Actos), Rosiglitazone (Avandia):
- Mechanism: Increases insulin sensitivity by activating peroxisome proliferator-activated receptor-gamma (PPAR-γ) in adipose tissue, muscle, and liver, enhancing glucose uptake without increasing insulin secretion.
- Side Effects: Fluid retention, leading to edema and worsening heart failure. Rosiglitazone is associated with increased cardiovascular events (MI), while Pioglitazone has a possible link to bladder cancer.
- α-Glucosidase Inhibitors - Acarbose (Precose), Miglitol (Glyset):
- Mechanism: Inhibits α-glucosidase enzymes in the intestinal brush border, delaying the breakdown of carbohydrates and slowing glucose absorption, reducing postprandial hyperglycemia.
- Side Effects: GI-related symptoms such as flatulence, diarrhea, and abdominal discomfort. May increase liver enzymes (LFTs) and in rare cases cause hepatitis.
- Meglitinides - Repaglinide (Prandin), Nateglinide (Starlix):
- Mechanism: Short-acting insulin secretagogues that stimulate insulin release from the pancreas in response to meals, providing flexible postprandial glucose control.
- Side Effects: Hypoglycemia, though less severe than with sulfonylureas due to the shorter action. Weight gain is also common.
- GLP-1 Receptor Agonists - Exenatide (Byetta, Bydureon), Liraglutide (Victoza, Saxenda), Dulaglutide (Trulicity), Semaglutide (Ozempic, Rybelsus):
- Mechanism: Mimics the action of the incretin hormone GLP-1, stimulating insulin secretion in a glucose-dependent manner, reducing glucagon secretion, and slowing gastric emptying, leading to improved glycemic control and weight loss.
- Side Effects: Common GI side effects such as nausea and vomiting due to delayed gastric emptying. Risk of hypoglycemia when combined with insulin or sulfonylureas. Caution in patients with gastroparesis.
- DPP-4 Inhibitors - Sitagliptin (Januvia), Saxagliptin (Onglyza), Linagliptin (Tradjenta), Alogliptin (Nesina):
- Mechanism: Inhibits dipeptidyl peptidase-4 (DPP-4), which degrades incretin hormones such as GLP-1, leading to prolonged action of endogenous incretins, enhancing glucose-dependent insulin release and suppressing glucagon secretion.
- Side Effects: May cause pancreatitis and joint pain. Potential risk of renal dysfunction, particularly in patients with pre-existing renal disease. Saxagliptin has been associated with an increased risk of heart failure.
- SGLT2 Inhibitors - Canagliflozin (Invokana), Dapagliflozin (Farxiga), Empagliflozin (Jardiance), Ertugliflozin (Steglatro):
- Mechanism: Inhibits sodium-glucose co-transporter-2 (SGLT2) in the proximal renal tubules, preventing glucose reabsorption and increasing glucose excretion in urine, leading to decreased blood glucose levels and weight loss.
- Side Effects: Increased risk of genital mycotic infections, urinary tract infections, and dehydration. May also cause euglycemic diabetic ketoacidosis (DKA) and an increased risk of lower limb amputations (especially with Canagliflozin).
Summary of Mechanisms and Key Side Effects:
- Metformin: Reduces hepatic glucose production; risk of lactic acidosis
- Sulfonylureas: Stimulates insulin release; risk of hypoglycemia, weight gain
- Thiazolidinediones: Increases insulin sensitivity; risk of fluid retention, cardiovascular issues
- α-Glucosidase Inhibitors: Delays glucose absorption; GI side effects.
- Meglitinides: Stimulates meal-time insulin release; risk of hypoglycemia, weight gain
- GLP-1 Agonists: Mimics incretin, promotes insulin release; GI side effects, hypoglycemia with other agents
- DPP-4 Inhibitors: Prolongs incretin activity; risk of pancreatitis, joint pain, heart failure
- SGLT2 Inhibitors: Increases glucose excretion via urine; risk of UTIs, ketoacidosis, amputations
Normal fasting glucose is between 70 and 100
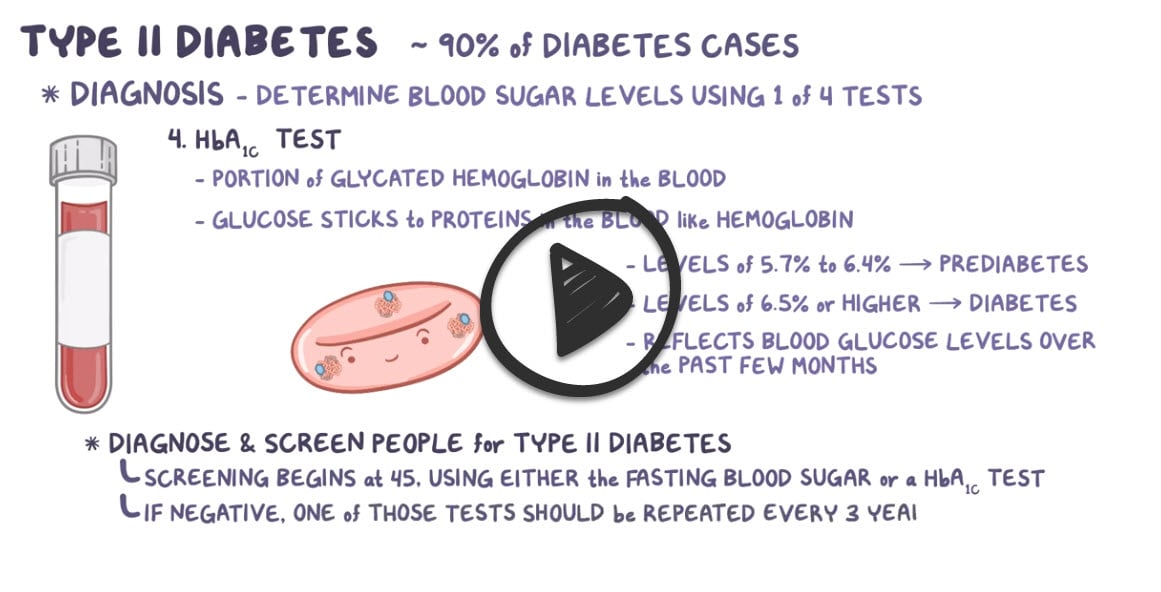
- A1C ≥ 6.5%
- FPG ≥ 126 mg/dL (fasting is defined as no caloric intake for at least 8 hours)
- 2-hour plasma glucose ≥ 200 mg/dL during an OGTT – glucose load containing the equivalent of 75 g anhydrous glucose dissolved in water
- Random plasma glucose ≥ 200 mg/dL in a patient with classic symptoms of hyperglycemia or hyperglycemic crisis
- A1C 5.7 to 6.4%
- FPG 100 to 125 mg/dL
- 2-hour post-load glucose on the 75 g OGTT 140 to 199 mg/dL
If the diagnostic test is consistent with prediabetes, it should be repeated annually

"Did you know?Symptomatic patients (polyuria, polydipsia, weight loss, blurry vision, or hyperglycemic crisis):
- A single abnormal value (e.g., random glucose ≥ 200 mg/dL) is sufficient to diagnose diabetes.
Asymptomatic patients: Two abnormal test results are required — either
- Two different tests from the same blood draw (e.g., A1C and fasting glucose), or
- The same test was repeated on a different day.
- If two tests are discordant, the abnormal test must be repeated and confirmed."
A C-peptide test is often used to help tell the difference between type 1 and type 2 diabetes
- C-peptide is a substance made in the pancreas, along with insulin. C-peptide and insulin are released from the pancreas at the same time and in about equal amounts. So a C-peptide test can show how much insulin your body is making
- With type 1 diabetes, your pancreas makes little to no insulin, and little or no C-peptide = ↓ C-peptide
- With type 2 diabetes, the body makes insulin but doesn't use it well. This can cause ↑ C-peptide
Diet and exercise with lifestyle changes are first-line - carbs 50-60% and protein 15-20%
- Studies demonstrate that just 150 minutes (2.5 hours) per week of moderate to vigorous exercise significantly reduces microvascular complications, including retinopathy, in patients with T2D
| Patient Profile | Preferred Add-on Agent | Key Benefit |
|---|---|---|
| Established ASCVD | GLP-1 Receptor Agonists | Reduced MACE (Major Adverse Cardiovascular Events) |
| Heart Failure (HFrEF) | SGLT2 Inhibitors | Reduced HF Hospitalization |
| CKD | SGLT2 Inhibitors | Renoprotection / Reduced Proteinuria |
| Weight Loss Priority | Tirzepatide / GLP-1 Agonists | Significant Weight Reduction |
Glucose goals and management
- A1C < 7.0 % check every 3 months if not controlled or if therapy has changed/requires adjustment and 2 x per year if controlled
- Preprandial glucose 80-130 mg/dL (60-90 if pregnant)
- Peak postprandial (1 to 2 hours after the beginning of the meal) blood glucose < 180 mg/dL
- Annual dilated eye exams, ACEI if microalbuminuria, annual foot examination
| Intervention | Expected A1C Decrease (%) | Advantages | Disadvantages |
| Lifestyle changes
(weight loss/activity) |
1.0 to 2.0 | Broad health benefits, no cost | Often insufficient alone within the first year due to inadequate weight loss or regain |
| Metformin
(generic: metformin, trade: Glucophage) |
1.0 to 2.0 | Weight loss to weight neutral, low cost, low hypoglycemia risk, well-tolerated, effective in combination | GI side effects, contraindicated in renal impairment (eGFR <30 mL/min) |
| Insulin (intermediate/long-acting)
(ex: Insulin glargine [Lantus], Insulin detemir [Levemir]) |
1.5 to 3.5 | Unlimited dose flexibility, rapid glucose control, potential lipid profile improvement | Multiple injections, weight gain, hypoglycemia, requires monitoring, high cost (especially analogs) |
| Dual GLP-1 and GIP receptor agonist
(ex: Tirzepatide [Mounjaro]) |
2.0 to 2.5 | Weight loss | Requires injection, frequent GI side effects, very expensive |
| GLP-1 receptor agonist (oral/injection)
(ex: Liraglutide [Victoza], Semaglutide [Ozempic], Dulaglutide [Trulicity]) |
0.5 to 2.0 | Weight loss, reduces major adverse cardiovascular events in high-risk patients | Injection often required, frequent GI side effects, high cost |
| SGLT2 inhibitor
(ex: Empagliflozin [Jardiance], Canagliflozin [Invokana], Dapagliflozin [Farxiga]) |
0.5 to 0.7 | Weight loss, lowers blood pressure, reduces heart failure and cardiovascular death, improves kidney function | Risk of mycotic infections, diabetic ketoacidosis, UTI, bone fractures, lower limb amputations |
| Sulfonylurea
(ex: Glipizide [Glucotrol], Glyburide [Diabeta], Glimepiride [Amaryl]) |
1.0 to 2.0 | Rapidly effective | Weight gain, risk of hypoglycemia |
| Thiazolidinedione
(ex: Pioglitazone [Actos], Rosiglitazone [Avandia]) |
0.5 to 1.4 | Improved lipid profile (pioglitazone), possible MI risk reduction (pioglitazone) | Fluid retention, heart failure, weight gain, bone fractures, possible MI risk (rosiglitazone), bladder cancer |
| Meglitinides
(ex: Repaglinide [Prandin], Nateglinide [Starlix]) |
0.5 to 1.5 | Rapid glucose control | Weight gain, requires thrice-daily dosing, risk of hypoglycemia |
| DPP-4 inhibitor
(ex: Sitagliptin [Januvia], Saxagliptin [Onglyza], Linagliptin [Tradjenta]) |
0.5 to 0.8 | Weight neutral | Long-term safety uncertain, expensive, potential increased heart failure risk with saxagliptin |
| Alpha-glucosidase inhibitor
(ex: Acarbose [Precose], Miglitol [Glyset]) |
0.5 to 0.8 | Weight neutral | Frequent GI side effects, requires thrice-daily dosing |
| Table adapted from UpToDate | |||
| Insulins | ||||
 Image by A. Peters, M. Komorniczak. License: CC BY 3.0 |
||||
| Insulin effect | Type of Insulin | Onset of action | Peak of action | Duration of action |
| Fast acting | Lispro | 15–30 minutes | 1–3 hours | 4–6 hours |
| Aspart | ||||
| Glulisine | ||||
| Short-acting | Regular | 30 minutes | 1.5–3.5 hours | 8 hours |
| Intermediate-acting | NPH | 1–2 hours | 4–6 hours | > 12 hours |
| Long-acting | Detemir | 1–2 hours | 3–9 hours | 14–24 hours |
| Glargine | 3–4 hours | No peak | Approximately 24 hours | |
| Degludec | Approximately 1 hour | No peak | > 40 hours | |
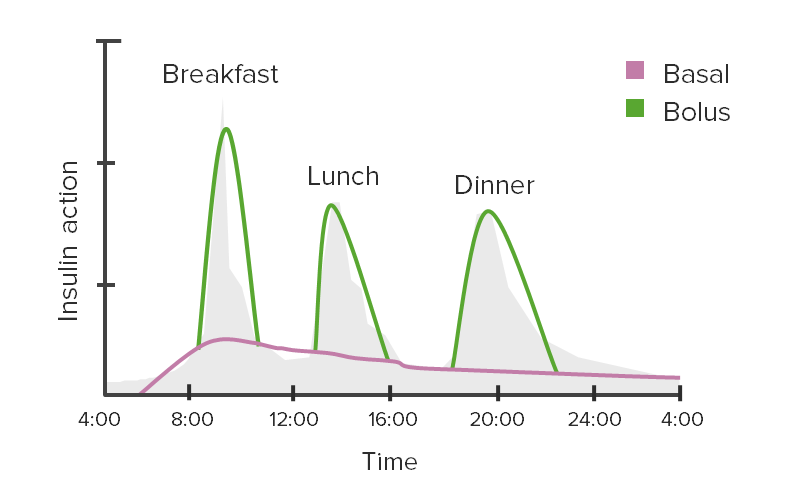
Example of insulin regimen:
|
||||
Blood pressure
- JNC 8 treatment targets: Reduce BP to < 140/90 mm Hg for everyone < 60, including those with a kidney disorder or diabetes
- ADA recommends treating BP of <140 and <90 mmHg. Lower treatment targets, i.e., 130/80 mmHg, may be appropriate for individuals at high risk of CVD, if they can be achieved without undue treatment burden.
- ACC/AHA blood pressure targets - target for patients with comorbidities: < 130/80
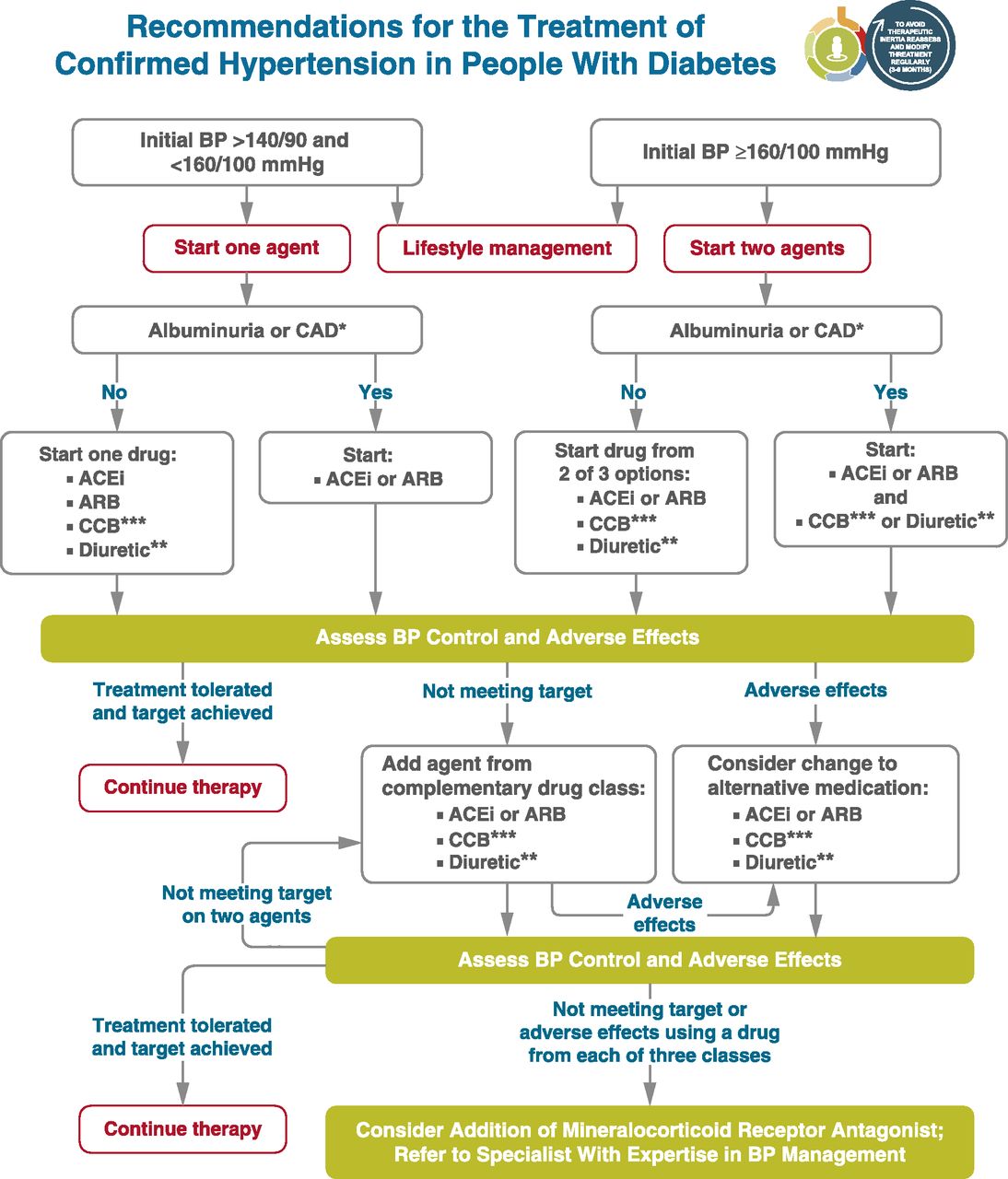 From ADA Standards - Section 10, CV Disease **Thiazide-like diuretics; long-acting agents shown to reduce cardiovascular events, such as chlorthalidone and indapamide, are preferred. ***Dihydropyridine calcium channel blocker (CCB). |
Cholesterol
- New statin guidelines recommend statins in all persons with diabetes mellitus who are 40 to 75 years of age with LDL-C levels of 70 to 189 mg per dL but without clinical ASCVD (see guidelines)
|
High, Moderate, and Low-Intensity Statin Therapy |
||
|---|---|---|
| High Intensity | Moderate Intensity | Low Intensity |
| Daily dosage lowers LDL-C by approximately ≥ 50% on average | Daily dosage lowers LDL-C by approximately 30% to 50% on average | Daily dosage lowers LDL-C by < 30% average |
| Atorvastatin (Lipitor), 40 to 80 mg | Atorvastatin, 10 (20) mg | Simvastatin, 10 mg |
| Rosuvastatin (Crestor), 20 (40) mg | Rosuvastatin, (5) 10 mg | Pravastatin, 10 to 20 mg |
| Simvastatin (Zocor), 20 to 40 mg | Lovastatin, 20 mg | |
| Pravastatin (Pravachol), 40 (80) mg | Fluvastatin, 20 to 40 mg | |
| Lovastatin (Mevacor), 40 mg | Pitavastatin, 1 mg | |
| Fluvastatin XL (Lescol XL), 80 mg | ||
| Fluvastatin, 40 mg twice daily | ||
| Pitavastatin (Livalo), 2 to 4 mg | ||
Aspirin
- Aspirin (75 to 162 mg/day) is recommended for secondary prevention in diabetic patients with a history of MI, vascular bypass, stroke or transient ischemic attack, peripheral vascular disease, claudication, or angina
- For the primary prevention of ASCVD in patients with diabetes at increased cardiovascular risk (10-year risk >10 percent), we suggest aspirin (75 to 162 mg daily)
- Prevention of ASCVD in adults with diabetes at low risk (10-year ASCVD risk <10 percent) is not routinely recommended
Vaccination
- Influenza: Yearly for all adults. ≥65 years: High-dose or adjuvanted vaccine preferred
- Pneumococcal:
- Age ≥65 or with diabetes: PCV20 (1 dose) or PCV15 + PPSV23 (1 year later)
- Age 19–64 with diabetes: PCV20 or PCV15 + PPSV23
- Hepatitis B: Unvaccinated adults <60 years: Complete series (2–3 doses). ≥60 years: Recommended for diabetes or other risks
- Hepatitis A: Unvaccinated adults with diabetes, chronic liver disease, or other risk factors: Complete 2-dose series (0 and 6–12 months)
- COVID-19: All adults: Stay up to date with the latest CDC-recommended primary series and boosters (e.g., 2024–2025 updated vaccine).
- Tetanus/Diphtheria/Pertussis: Tdap once, then Td or Tdap every 10 years
- Herpes Zoster: ≥50 years: Shingrix (2 doses, 2–6 months apart)
Monitoring in patients with diabetes mellitus (summary table)
| History and physical examination | ||
| Height, weight, and BMI | Every visit | |
| Smoking cessation counseling | Every visit | For smokers only. |
| Blood pressure | Every visit | Goal systolic pressure 125 to 130 mmHg. |
| Dilated eye examination | Annually | Begin at onset of type 2 diabetes, 3 to 5 years after onset of type 1 diabetes. Examine yearly (or more frequently) if retinopathy is present, every 2 to 3 years if there is no evidence of retinopathy. |
| Comprehensive foot examination | Annually | Every visit if peripheral vascular disease or neuropathy. |
| Dental examination | Annually | Periodontal disease is more severe but not necessarily more prevalent in patients with diabetes. |
| Laboratory studies | ||
| Lipid profile | Initially, as indicated | In people without dyslipidemia and not on cholesterol-lowering therapy, testing may be infrequent. |
| A1C | Every 3 to 6 months | Goal ≤ 7% (may be lower or higher in selected patients). |
| Urinary albumin-to-creatinine ratio | Annually | Begin 3 to 5 years after onset of type 1 diabetes and at diagnosis in patients with type 2 diabetes; protein excretion should also be monitored if persistent albuminuria is present. |
| Serum creatinine | Initially, as indicated | Typically annually; more often in the presence of chronic kidney disease. |
| Vaccinations | ||
| Pneumococcus | ||
|
1 dose, ages 19 to 64 years | Once the patient is ≥ 65 years (and ≥1 year after PCV13 and > 5 years after previous dose of PPSV23), give a second dose of PPSV23. Revaccinate every 10 years. |
|
1 dose at age ≥ 65 years | Once the patient is ≥65 years (and ≥1 year after PPSV23), give PCV13. |
|
1 dose, ages 19 to 64 years or ≥ 65 years if no prior dose. No additional pneumococcal vaccine is needed! | |
| Influenza | Annually | |
| Hepatitis B | 3-dose series | Administer to unvaccinated adults who are ages 19 to 59 years. For older patients, administer based upon risk of acquiring hepatitis B, including the need for assisted blood glucose monitoring and the likelihood of an adequate immune response to vaccination. |
| Provide other routine vaccinations for adults with diabetes according to age-related recommendations. | ||
| Education, self-management review | ||
| Annually | More often at onset of diabetes and when there is a change in regimen. | |
 Osmosis Osmosis |
|
 |
Metformin is part of the Biguanide class of diabetic drugs. It is the first-line medical treatment for diabetes mellitus type 2 and can also be used for PCOS. Its exact mechanism of action is unknown, but this medication leads to decreased gluconeogenesis and increased insulin sensitivity, subsequently equating to lower blood sugar levels. Side effects of this drug include lactic acidosis and GI distress, and Metformin should not be used in patients with renal failure.
Play Video + QuizInsulins
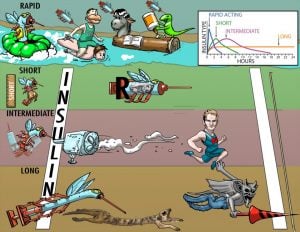
Insulins for medical use are synthetically created analogs of the human hormone. Some are chemically altered in structure to change the rate of absorption and duration of action within the human body. When classified according to time course, insulin preparations fall into three major groups: short duration, intermediate duration, and long duration.
Glyburide and Glipizide (2nd Generation Sulfonylureas)
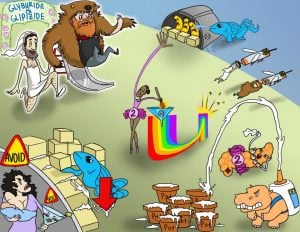
Glyburide and glipizide are second-generation sulfonylureas that stimulate the release of insulin from pancreatic islet cells. This action increases the amount of circulating insulin to maintain normal blood glucose levels in the body. These drugs are indicated for patients with type 2 diabetes who have the ability to produce insulin (refer to Picmonic “Insulin”). Second-generation sulfonylureas have replaced first-generation agents due to their increased potency and fewer drug-drug interactions. Hypoglycemia is a major side effect. These drugs should not be used while consuming alcohol and 2nd generation sulfonylureas (except glyburide) should not be used in pregnancy or breastfeeding.
Play Video + QuizGlucagon (GlucaGen)

Glucagon (GlucaGen) is a polypeptide hormone that causes the hepatic conversion of stored glycogen into readily-available glucose. This medication is indicated for hypoglycemia caused by insulin overdose and not related to starvation. It is given when IV glucose is not available. Side effects may include nausea and vomiting. This drug must be reconstituted with a powder supplied by the manufacturer. Once conscious, the patient should be given oral carbohydrates within an hour to avoid rebound hypoglycemia. If the patient shows no improvement, IV 50% glucose may be given for immediate results.
Play Video + QuizExenatide (Byetta)
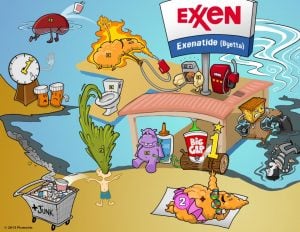
Exenatide (Byetta) is an injectable hypoglycemic drug indicated for patients with Type 2 diabetes. The medication functions as an incretin mimetic and GLP-1 synthetic analog. Side effects include hypoglycemia, nausea, vomiting, diarrhea, pancreatitis, and renal failure. Since exenatide delays gastric emptying, it should be administered at least 1 hour after giving other medications. Exenatide is considered adjunct therapy and administered with other antidiabetic drugs.
Play Video + QuizChlorpropamide and Tolbutamide (Orinase) (1st Generation Sulfonylureas)

Chlorpropamide and tolbutamide are first-generation sulfonylureas that promote insulin release. This action increases the amount of circulating insulin to maintain normal blood glucose levels in the body. These drugs are indicated for patients with type 2 diabetes who have the ability to produce insulin (refer to Picmonic “Insulin”). However, first-generation sulfonylureas are rarely used due to their lower potency and significant drug-drug interactions. Side effects of these medications include hypoglycemia and cardiovascular toxicity. These drugs should not be used while pregnant, breastfeeding, consuming alcohol, or taking beta-blockers.
Play Video + QuizAcarbose (Precose) and miglitol (Glyset)

Acarbose (Precose) and miglitol (Glyset) are alpha-glucosidase inhibitors used to help control blood glucose levels in diabetic patients. By inhibiting an intestinal enzyme that converts complex carbohydrates into digestible forms, these medications decrease the rate of carbohydrate digestion and absorption. This action decreases the rise of glucose levels caused by eating. These medications are indicated for patients with type 2 diabetes. Side effects include flatulence, cramps, diarrhea, and anemia. Since these drugs may cause liver damage, liver function tests should be monitored frequently. In the event of hypoglycemia, glucose (not sucrose) should be administered.
Play Video + QuizPioglitazone (Thiazolidinediones)

Pioglitazone stimulates receptors in the body to increase cellular response to insulin, thus decreasing insulin resistance. This medication is only effective in the presence of insulin and can only be used in patients with type II diabetes. Side effects of pioglitazone include upper respiratory infection, muscle pain, sinusitis, headache, and heart failure. Patients taking pioglitazone are at increased risk for bladder cancer, and women taking this medication are more prone to bone fractures. Liver enzymes should be routinely monitored while taking pioglitazone due to the risk of liver toxicity.
Play Video + QuizPramlintide (Symlin)

Pramlintide (Symlin) is an injectable hypoglycemic drug indicated for type 1 and 2 diabetes. As a synthetic amylin analog, pramlintide is used to supplement mealtime insulin in diabetic patients unable to maintain glucose control despite insulin therapy. Side effects of pramlintide include nausea and reactions at the injection site. While administering the medication, monitor the patient for symptoms of hypoglycemia. Since it delays the absorption of other medications, avoid giving pramlintide concurrently with other drugs.
Play Video + QuizRepaglinide (Prandin) and nateglinide (Starlix)

Repaglinide (Prandin) and nateglinide (Starlix) are oral hypoglycemic medications classified as meglitinides or “glinides.” By stimulating the pancreatic cells to release more insulin, these medications decrease blood glucose levels. A major side effect of meglitinides is hypoglycemia. Since these drugs have a short half-life, instruct the patient to eat within 30 minutes of administration. Gemfibrozil (Lopid) decreases the metabolism rate of meglitinides and should not be administered to prevent drug accumulation leading to hypoglycemia.
Play Video + QuizSitagliptin (Januvia) and Saxagliptin (Onglyza) (DPP-4 Inhibitors)
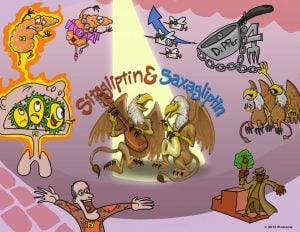
Sitagliptin (Januvia) and Saxagliptin (Onglyza) are antidiabetic medications that work by blocking the DPP-4 enzyme, allowing for increased action of incretin hormones and increased release of insulin. These medications are only effective in the presence of insulin and can only be used in patients with type II diabetes. Keep in mind, however, DPP-4 inhibitors are considered third-line medications for the treatment of diabetes and should only be used if first and second-line medications have failed to provide adequate blood glucose control. Side effects include upper respiratory infection, pancreatitis, and hypersensitivity reactions.
Play Video + QuizQuestion 1 |
acarbose Hint: α-Glucosidase inhibitors, such as acarbose (Precose), reduce glucose by delaying carbohydrate absorption | |
glipizide Hint: Glipizide (Glucotrol) and other sulfonylureas work by increased insulin secretion from pancreatic β cells. | |
metformin Hint: Metformin (Glucophage), a biguanide, lowers glucose by decreasing hepatic glucose production and increasing glucose utilization. | |
Pioglitazone |
Question 2 |
glucagon Hint: Glucagon would further increase the blood glucose | |
insulin Hint: Insulin is typically not needed unless the glucose is resistant to fluids | |
bicarbonate Hint: Bicarbonate should not be administered because the blood pH is above 7.0 | |
saline |
|
List |
References: Merck Manual · UpToDate