
Patient will present as → a 57-year-old male presents with complaints of fatigue, nausea, and headache that have developed over the past several weeks. His past medical history is significant for hypertension, diabetes mellitus, CHF, and small-cell lung cancer diagnosed and treated four years previously. Vital signs are as follows: T 37.3 °C, HR 82, BP 142/86, RR 16, O2Sat 97% on RA. On physical exam, peripheral edema is absent, and he is alert and oriented to person, place, and time. Abnormalities noted on initial labwork include glucose 138 mg/dL and sodium 122 mEq/L. Follow-up testing reveals a urine osmolality of 310 mmol/kg and a serum osmolality of 268 mmol/kg; BUN and creatinine levels are within normal limits.
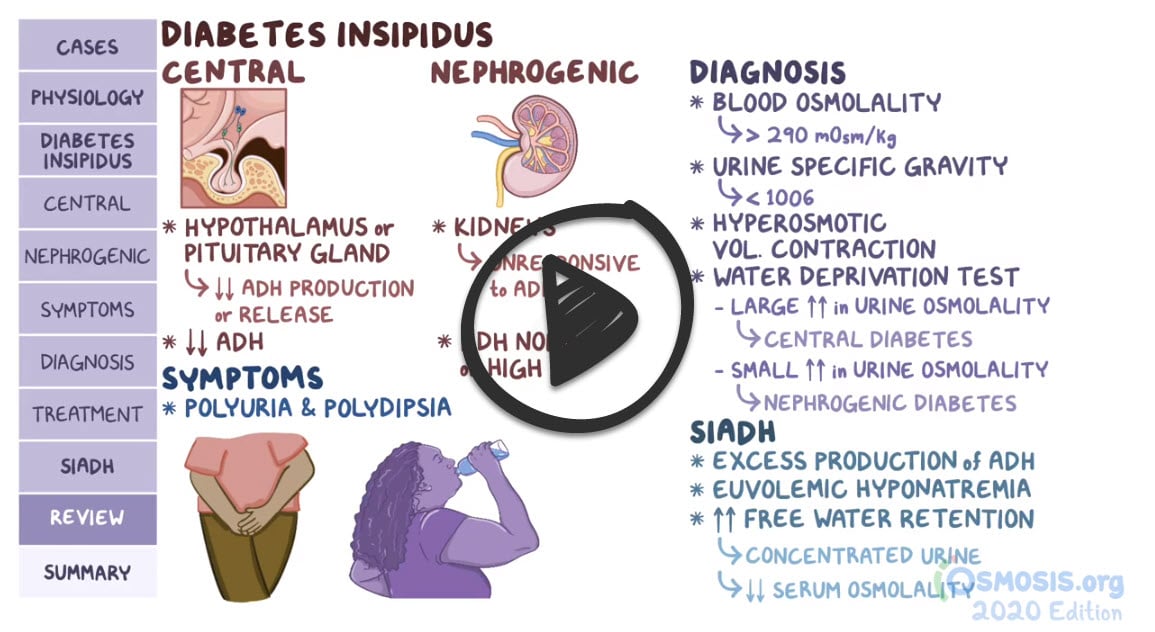
Syndrome of inappropriate antidiuresis (SIAD), the more current term for what is also known as the syndrome of inappropriate antidiuretic hormone (SIADH), is characterized by excessive release of antidiuretic hormone (ADH) from the posterior pituitary, resulting in the kidneys retaining water, even when the body doesn't need it. This leads to:
-
- Dilution of serum: There's too much water in relation to sodium and other electrolytes, making the blood overly dilute -> Presents with hyponatremia
- Concentrated urine: Because the kidneys are reabsorbing water, the urine becomes abnormally concentrated
- Symptoms can vary depending on how rapidly the condition develops. In some cases, nausea and vomiting, headache, confusion, weakness, and fatigue may be experienced
Causes of inappropriate ADH release include:
- Malignancy - small cell (oat cell) carcinoma of the lung
- Medications - carbamazepine, cyclophosphamide, nonsteroidal anti-inflammatory drugs (NSAIDs), sulfonylureas, and selective serotonin reuptake inhibitors (SSRIs)
- Central nervous system (CNS) disturbances - infection (encephalitis and meningitis), malignancy, stroke (hemorrhagic and ischemic)
- Traumatic brain injury
- Pulmonary disturbances - pneumonia, tuberculosis
Patients at greater risk for SIADH include those with malignant, CNS, and pulmonary disease
- In nursing homes, on medications that enhance ADH activity
- Hospitalized patients - particularly on mechanical ventilation
- Hyponatremia with low plasma osmolality (<275 mOsm/kg)
- Inappropriately concentrated urine (urine osmolality >100 mOsm/kg)
- Elevated urine sodium (>40 mEq/L)
- Normal adrenal and thyroid function to exclude other causes
Serum studies
- ↓ serum sodium (< 135 mmol/L)
- ↓ plasma osmolality (< 275 mOsm/kg)
- ↓ serum uric acid (< 4 mg/dL)
- Normal adrenal and thyroid function
Urine studies
- ↑ urine sodium (> 40 mmol/L)
- ↑ urine osmolality (> 100 mOsm/kg)
Fluid restriction as the first-line treatment
- Sodium management is dependent on symptom severity and duration of hyponatremia
- Severe symptoms - hypertonic (3%) saline—give carefully to avoid central pontine myelinolysis (CPM), also known as osmotic demyelination syndrome (a complication of correcting serum Na+ too quickly causing damage to the myelin sheath in the brain )
- Mild-to-moderate symptoms - isotonic (0.9%) saline with furosemide
Medications - vaptans (ADH receptor antagonist) - e.g., tolvaptan and conivaptan
- Demeclocycline (ADH receptor antagonist)
- Lithium (decreases responsiveness to ADH)
 Osmosis Osmosis |
|
 |

Syndrome of inappropriate antidiuretic hormone (SIADH) occurs when antidiuretic hormone (ADH) which normally regulates the retention of water by the kidneys is secreted in inappropriately increased amounts. This could be ectopically from things like cancers, especially small cell lung tumors. This can also occur as a side effect of some drugs, like the cancer drugs cyclophosphamide, and antidiabetic medications, such as the first generation sulfonylureas, as well as some seizure medications. In some instances, SIADH could be triggered by head trauma, stroke, or some diseases, like HIV. The assessment of SIADH will present as a patient with volume overload, as the kidneys will retain excess water and cause fluid shifts within patient tissue compartments.
Play Video + QuizSIADH Nonpharmacologic Interventions

Syndrome of Inappropriate Antidiuretic Hormone (SIADH) occurs when antidiuretic hormone (ADH) which normally regulates the retention of water by the kidneys is secreted in inappropriately increased amounts. Treatment of SIADH is aimed at correcting dilutional hyponatremia, closely monitoring for electrolyte and weight changes, as well as administering medications to decrease fluid retention. This card will cover the nonpharmacologic interventions of monitoring of serum and urine osmolality, recording I’s and O’s with daily weights, restriction of fluid intake, monitoring of cardiovascular and neurological status, as well as initiating seizure precautions.
SIADH Pharmacologic Interventions

Syndrome of Inappropriate Antidiuretic Hormone (SIADH) occurs when antidiuretic hormone (ADH) which normally regulates the retention of water by the kidneys is secreted in inappropriately increased amounts. Treatment of SIADH is aimed at correcting dilutional hyponatremia, closely monitoring for electrolyte and weight changes, as well as administering medications to decrease fluid retention. This card will cover the pharmacologic interventions, which include administration of diuretics, hypertonic IV fluids, and the medications Demeclocycline, Tolvaptan, and Conivaptan.
Play Video + QuizQuestion 1 |
High serum sodium, high serum osmolality, low urine osmolality | |
High serum sodium, high serum osmolality, high urine osmolality | |
Low serum sodium, low serum osmolality, low urine osmolality | |
Low serum sodium, low serum osmolality, high urine osmolality | |
None of the above |
References: Merck Manual · UpToDate