Patient will present as → a 23-year-old female with a one-week history of cough productive of whitish sputum. This was preceded one week prior by a URI. She denies chills, night sweats, shortness of breath, or wheeze. Temperature is 99.9°F (37.7°C).
Patient will present as → a 5-year-old boy who is brought to the emergency department by his parents for a cough and shortness of breath. He has a past medical history of eczema and seasonal rhinitis.On physical exam, you note a young boy in respiratory distress, taking deep, slow breaths to try to catch his breath. He has diminished breath sounds in all lung fields with prolonged expiratory wheezes.
Presentation: Most often, young patients present with wheezing and dyspnea, often associated with illness, exercise, and allergic triggers
Airway inflammation, hyperresponsiveness, and reversible airflow obstruction
Diagnosis and monitor with peak flow. PFTs: Greater than 12% increase in FEV1 after bronchodilator therapy
FEV1/FVC ratio < 0.70 (You would expect the amount of air exhaled during the first second (FEV1) to be the greatest amount
In asthma, since there is an obstruction (inflammation), you will have a decreased FEV1 and therefore a reduced FEV1 to FVC ratio
Acute treatment: Oxygen, nebulized SABA, ipratropium bromide, and oral corticosteroids
Low-dose ICS with rapid onset LABA (eg, budesonide-formoterol combination MDI 160 mcg-4.5 mcg/inhalation or DPI 200 mcg-6 mcg/inhalation) 1 inhalation, as needed
or
Low-dose ICS whenever SABA used
Step 2
Asthma symptoms or need for reliever inhaler ≥2 times/week
Low-dose ICS daily, with SABA as needed (preferred)
or
Low dose ICS-formoterol as needed (preferred)
Other options
Low-dose ICS plus SABA, concomitantly administered, as needed
or (less preferred)
LTRA daily and SABA as needed
Step 3
Troublesome asthma symptoms most days, nocturnal awakening due to asthma ≥1 time/month, risk factors for exacerbations¶
Low-dose ICS-LABA as maintenance and reliever therapy (ie, budesonide-formoterol) (preferred)
or
Low-dose ICS-LABA combination daily, with SABA as needed
Other options
Medium-dose ICS daily, with SABA as needed
or
Low-dose ICS plus LTRA daily, with SABA as needed
Steps 4 to 5
Severely uncontrolled asthma with ≥3 of the following: daytime asthma symptoms >2 times/week; nocturnal awakening due to asthma; reliever needed for symptoms >2 times/week, or activity limitation due to asthma
or
An acute exacerbation
Step 4:
Medium-dose ICS-LABA daily and SABA as needed
Other options
High-dose ICS daily – May need short course of oral glucocorticoids
Possible add-on tiotropium, LTRA
Step 5:
High-dose ICS-LABA daily and SABA as needed (preferred)
Assess for possible add-on therapy (eg, tiotropium, zileuton, anti-IgE, anti-IL-5, anti-IL-5R, anti-IL-4R)
Other options
Oral glucocorticoids titrated to optimize asthma control and minimize adverse effects
Forced expiratory volume (FEV) measures how much air a person can exhale during a forced breath. The amount of air exhaled may be measured during the first (FEV1), second (FEV2), and/or third seconds (FEV3) of the forced breath. Forced vital capacity (FVC) is the total amount of air exhaled during the FEV test
You would expect the amount of air exhaled during the first second to be the greatest amount. In asthma, since there is an obstruction (inflammation) you will have a decreased FEV1 and therefore a reduced FEV1 to FVC ratio.
Patient will present as → a 25-year-old cystic fibrosis patient complaining of chronic, frequent coughing productive of yellow and green sputum. She recently recovered from a Pseudomonas spp. Pneumonia requiring hospitalization. On physical examination, you notice foul breath, purulent sputum, and hemoptysis, along with a CXRdemonstrating dilated and thickened airways with “plate-like” atelectasis (scarring).
A condition in which the lungs' airways become dilated and damaged, leading to inadequate clearance of mucus in airways
Mucus builds up and breeds bacteria, causing frequent infections - crackles, wheezes, purulent sputum
A common endpoint of disorders that cause chronic airway inflammation (CF, immune defects, recurrent pneumonia, aspiration, tumor)
Symptoms include a daily cough that occurs over months or years, production of copious foul-smelling sputum, and frequent respiratory infections
DX: CXR = linear “tram track” lung markings, dilated and thickened airways – “plate-like” atelectasis
CT chest = gold standard
TX: ambulatory oxygen, aggressive antibiotics for acute exacerbations, CPT (chest physiotherapy = bang on the back); eventual lung transplant
Chest X-ray of hyperinflated lung with bronchiectasis at the right upper lobe of a 12-year-old boy.
A CT scan demonstrating very pronounced bronchiectasis in a 75-year-old man, especially on the right (left in the picture). There is a florid superinfection with a large accompanying effusion
Patient will present with → a 43-year-old man who comes to the emergency department because of a 3-week history of episodic cutaneous flushing, diarrhea, and wheezing. He has a past medical history of hypertension and type 2 diabetes mellitus. His temperature is 36.6°C (97.9°F), pulse is 125/min, respirations are 30/min, and blood pressure is 90/60 mm Hg. Pulmonary examination shows diffuse wheezes in both lung fields. Cardiac examination shows a prominent “v” wave of the jugular vein and a 1/6 holosystolic murmur best heard on the left lower sternal border. Abdominal examination shows hyperactive bowel sounds.
A tumor arising from neuroendocrine cells → leading to excess secretion ofserotonin, histamine, and bradykinin
Common primary sites include GI (small and large intestines, stomach, pancreas, liver), lungs, ovaries, and thymus
The most common site of a neuroendocrine (carcinoid) tumor to metastasize to is the liver
Carcinoid tumor of the appendix is the most common cause. The appendiceal cancer travels from the appendix then to the liver where it metastasizes to the lungs
Usually asymptomatic until liver metastasis; symptoms develop occasionally
GI tract tumor→ hormone secretion → enter into enterohepatic circulation → liver inactivates hormones → no symptoms
Liver tumor → hormone secretion → released into circulation + liver dysfunction → symptoms
Carcinoid syndrome (the hallmark sign) = Cutaneous flushing, diarrhea, wheezing and low blood pressure is actually quite rare and occurs in ~ 5% of carcinoid tumors and becomes manifest when vasoactive substances from the tumors enter the systemic circulation escaping hepatic degradation.
The syndrome includes flushing, ↑ intestinal motility (diarrhea), itching and less frequently, heart failure, vomiting, bronchoconstriction, asthma, and wheezing
↑ Serotonin leads to collagen fiber thickening, fibrosis = heart valve dysfunction → tricuspid regurgitation, pulmonary stenosis/bronchoconstriction, and wheezing
↑ Histamine and bradykinin = vasodilation and flushing
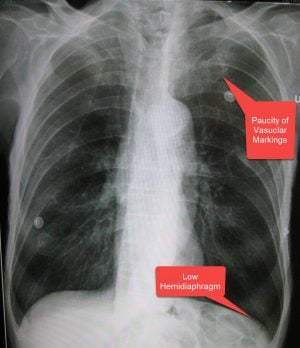
Patient will present as →a 56 yo female with shortness of breath, as well as a productive cough that has occurred over the past two years for at least three months each year. She is a heavy smoker. Physical exam reveals a respiratory rate of 32, slightly labored breathing, and a temperature of 98.9F. Her SpO2 is 90% while receiving oxygen via nasal cannula at 2 Lpm. (chronic bronchitis)
Chronic obstructive pulmonary disease ( COPD ) is a chronic inflammatory lung disease that causes obstructed airflow from the lungs due to loss of elastic recoil and increasing airways resistance
Includes emphysema and chronic bronchitis ⇒ both usually coexist with one being more dominant
Damage to the lungs from COPD can't be reversed
Risk factors:
Cigarette smoking/exposure is the most important risk
Alpha 1 antitrypsin deficiency = genetic and linked to COPD in patients < 40y/o (protects elastin in lungs from damage by WBCs)
≥20 pack-year history (ages 50–80, currently smoking or quit within 15 years) = low-dose chest CT
Exposure to irritants (e.g. cigarette smoke) → degrades elastin in alveoli, airways → lose elasticity → low pressure during expiration pulls walls of alveoli inward → collapse → air-trapping distal to collapse → septa breaks down → neighboring alveoli coalesce into larger air spaces → decreased surface area available for gas exchange
Loss of elastin → lungs are more compliant (lungs expand, hold air)
Alveolar air sacs permanently enlarge, lose elasticity → exhaling is difficult
DOE = hallmark symptom
Hyperinflation of lungs + hyperresonance to percussion, decreased/absent breath sounds, decreased fremitus, barrel chest (increased AP diameter), quiet chest, pursed-lip breathing
Individuals are able to oxygenate blood (pink) but they have to purse their lips to do so (puffers) = Pink Puffers!
Pursing lips increases pressure in the airway → keeps the airway from collapsing → weight loss
Barrel chest due to air trapping and hyperinflation of lungs
CXR reveals loss of lung markings, hyperinflation, and increased anterior-posterior diameter
PFTs show FVC decreased (esp. FEV1) + increased TLC (due to air trapping)
Defined as a chronic cough that is productive of phlegm occurring on most days for 3 months of the year for 2 or more consecutive years without an otherwise-defined acute cause
Exposure to irritants (e.g. cigarette smoke) → hypertrophy/hyperplasia of bronchial mucous glands, goblet cells in bronchioles, cilia less mobile → increased mucus production, less movement → mucus plugs → obstruction in bronchioles → air-trapping → productive cough
Smoking cessation = the single most important step
Bronchodilators: combo therapy β2 agonist + anticholinergic = greater response than used alone – tx of choice in stable COPD with resp. symptoms
Short-acting (SAMA) or long-acting (LAMA) muscarinic agent (also known as an anticholinergic agent): tiotropium (Spiriva) inhaled long-acting; ipratropium (Atrovent)
For maintenance, a long-acting muscarinic antagonist (LAMA, e.g., tiotropium) or LABA is preferred; short-acting agents (ipratropium/albuterol) are for rescue
Contraindications: severe CAD; caution in pt. with DM (hyperglycemia), hyperthyroid
Theophylline: only used in refractory cases due to narrow therapeutic index – monitor serum levels to prevent nausea, palpitations, arrhythmias, and seizures from toxic levels; higher doses needed in smokers and coffee drinkers- don’t initiate in acute exacerbation
+/- inhaled glucocorticoids: inhaled corticosteroids are not considered monotherapy
s/e: osteoporosis, thrush
Oxygen: only medical therapy proven to decrease mortality (decreases pulmonary hypertension/cor pulmonale by decreasing hypoxia-mediated pulmonary vasoconstriction)
Long-term oxygen therapy in all patients with COPD who have chronic hypoxemia defined as resting PaO2 < 55 mmHg or SaO2 <89%
Patient will present as → 65 y/o with 3 days of progressive dyspnea and purulent sputum production. The patient takes albuterol and tiotropium bromide for moderate COPD. His PMH is relevant for a 40 pack-year smoking history, type II DM, hyperlipidemia, and coronary artery stenting 2 years ago. PE shows barrel-shaped chest, inspiratory crackles, hepatojugular reflux, pulsus paradoxus, and ventricular gallop. His temperature is 38.1°C (100.5°F), his pulse is 130/min, respirations are 28/min, blood pressure is 130/84 mmHg, and pulse oximetry on room air shows an oxygen saturation of 86%.
Right ventricular enlargement and eventually failure secondary to lung disorder that causes pulmonary artery HTN
The diagnosis of cor pulmonale is usually made with an echocardiogram that shows evidence of increased pressure in the pulmonary arteries and right ventricle.
Follow-up tests can be done to identify the underlying cause, for example, spirometry can be done to look for chronic lung disease
The gold standard diagnostic test to directly measure pulmonary pressures and assess for response to vasodilating medications is a right heart catheterization.
TX: Diagnose and treat the underlying condition before cardiac structure change becomes irreversible
Diuretics are not helpful! May be harmful
Hypoventilation syndrome
Hypoventilation syndrome may be secondary to several mechanisms, including central respiratory drive depression (drugs -narcotics, benzodiazepines, neurologic disorders - multiple sclerosis, etc.), neuromuscular disorders (ALS, myasthenia gravis, etc.), chest wall abnormalities,obesity hypoventilation, and COPD
Obesity hypoventilation syndrome (OHS), also known as Pickwickian syndrome, is a condition in which severely overweight people fail to breathe rapidly or deeply enough, resulting in low oxygen levels and high blood carbon dioxide (CO2) levels.
Patient will present as →a 55-year-old female who is a current smoker presents with a 9-month history of respiratory symptoms, including dyspnea on exertion, thoracic pain, and dry cough, which were preceded by a pulmonary infection. On auscultation, you hear inspiratory crackles. Pulmonary function tests (PFTs) show only mild impairment of vital capacity with decreased lung volume and a normal to increased FEV1/FVC ratio.
Idiopathic pulmonary fibrosis (IPF) is a type of lung disease that results in scarring (fibrosis) of the lungs for an unknown reason
Over time, the scarring gets worse, and it becomes hard to take in a deep breath, and the lungs cannot take in enough oxygen
Etiology unknown; MC of all interstitial lung diseases
In order to be considered "idiopathic", you must rule out other common causes such as drugs (amiodarone), and environmental or occupational exposures
non-idiopathic: smoking, viral infections, environmental (silica, hard metal dust), medication, genetics, XRT, GERD
Patient will present as →a 53-year-old man presents to the office complaining of progressive dyspnea over the past few years. History reveals that he has worked in construction for the past 20 years demolishing and refurbishing old buildings. He rarely uses any protective breathing equipment. Physical examination demonstrates an afebrile man in mild respiratory distress with inspiratory crackles. The chest x-ray reveals a reticular linear pattern with basilar predominance, opacities, and honeycombing. (asbestosis)
Any fibrosis of the lung tissues with a known cause - usually from prolonged environmental or occupational contact
Patient will present as →a 71-year-old male who was admitted to the acute care hospital two days following a massive CVA with a possible brainstem infarct. Because he was also experiencing secondary respiratory failure, he was intubated and placed on mechanical ventilation. He was subsequently transferred to the neurointensive care unit where he was stabilized. His present vital signs are respiratory rate 14 (ventilator rate), temperature 100.4 F. His SpO2 is 95%. His rating on the Glasgow Coma Scale is 5.
Viral: adults ⇒ flu = MC cause; kids ⇒ RSV; comes on fast
Tx: voriconazole or isavuconazole (Aspergillus is intrinsically resistant to fluconazole)
Cryptococcus: found in soil; can disseminate and ⇒ meningitis
Lumbar puncture for meningitis
Tx: amphotericin B
Histoplasma capsulatum: pulmonary lesions that are apical and resemble cavitary TB; worsening cough and dyspnea, progression to disabling respiratory dysfunction; no dissemination
Bird or bat droppings (caves, zoo, bird); Mississippi Ohio River Valley
Signs: mediastinal or hilar LAD (looks like sarcoid)
Tx: amp B
HIV: PJP (pneumocystis jiroveci)
Common in HIV patients with a CD4 count <200
XR: diffuse interstitial or bilateral perihilar infiltrates
Dx: bronchoalveolar lavage PCR, labs, HIV test; low O2 sat despite supplemental oxygen
Tx: Bactrim and steroids; pentamidine for allergy
Prophylaxis for high-risk patients with CD4 <200 = daily Bactrim
CURB65: Estimates the mortality of community-acquired pneumonia to help determine inpatient vs. outpatient treatment
Confusion, urea > 7, RR > 30, SBP < 90 OR DBP < 60, age > 65
0-1 = low risk, consider home tx
2 = probable admission vs close outpatient management
Patient will present as → a 43-year-old woman with a history of COPD presents to the office with worsening dyspnea, especially at rest. She also complains of dull, retrosternal chest pain. On examination, she has persistent widened splitting of S2. Radiographic findings (seen here) demonstrate peripheral “pruning” of the large pulmonary arteries.
Blood pressure in the lungs is usually very low 15/5. In pulmonary hypertension, the pressure increases > 20 mmHg at rest
Usually caused by an underlying disorder (constrictive pericarditis, mitral stenosis = MC, LV failure, mediastinal disease, compression of pulmonary veins)
Mitral stenosis: mitral valve = tight, so blood can’t pass into the left ventricle ⇒ pressure backs up to the lungs
When the right heart can’t pump against vascular resistance ⇒ right heart failure = Cor pulmonale
Presentation: Dyspnea on exertion, fatigue, chest pain, edema
Physical Exam: Loud pulmonic component of second heart sound (P2); Jugular venous distension; Ascites; Hepatojugular reflux; Lower limb edema
Diagnose with a right heart catheterization (gold standard) → most accurate measure of pressures
Patient will present as→ a 65-year-old woman with a 40 pack-year history of smoking presents with a 7 kg weight lossover the last 3 months and recent onset of streaks of blood in the sputum. PE reveals a thin, afebrile woman with clubbing of the fingers, an increased anteroposterior diameter, scattered and coarse rhonchi and wheezes over both lung fields, and distant heart sounds.
Lung cancer is classified into 2 major categories
Small cell lung cancer (SCLC), about 15% of cases (poor prognosis)
Non–small cell lung cancer (NSCLC), about 85% of cases, includes four subtypes: adenocarcinoma, squamous cell carcinoma, large cell carcinoma, and carcinoid tumor
⇒ Small Cell (15% of cases) - 99% smokers, does not respond to surgery, and metastases at presentation
Location: (central mass), very aggressive
Treatment: Combination chemotherapy needed
Paraneoplastic syndromes: Cushing's, SIADH
⇒ Non-Small Cell (85% lung cancer cases)
Adenocarcinoma - most common (peripheral mass), 35-40% of cases of lung cancer
Most common
Associated with smoking and asbestos exposure
Location: Periphery
Paraneoplastic syndrome: Thrombophlebitis
Squamous cell (central mass) with hemoptysis, 25-35% of lung cancer cases
Location: central
May cause hemoptysis
Paraneoplastic syndrome: hypercalcemia
Elevated PTHrp
Large cell - fast doubling rates - responds to surgery, rare (only 5%)
Patient will present as → a 30-year-old African American female with a cough, fever, and generalized body aches. You order a CXR which shows bilateral hilar adenopathy.
Chronic autoimmune inflammatory disease in which small nodules (granulomas) develop in lungs, lymph nodes, and other organs
Pulmonary Manifestations (most common): Symptoms can include cough, dyspnea (difficulty breathing), and chest discomfort.
Pulmonary involvement is a hallmark of the disease and is often detected through imaging studies, such as chest X-rays or CT scans, which show bilateral hilar lymphadenopathy, pulmonary infiltrates, or nodules.
Skin Manifestations (2nd most common): It can present in various forms, including erythema nodosum (tender red nodules, usually on the lower legs), lupus pernio (chronic, violaceous, raised lesions on the face), and other dermatological presentations.
Symptoms vary, depending on the organs affected – fever, weight loss, arthralgias, erythema nodosum = initial presenting sx
Lupus pernio (chronic, violaceous, raised plaques and nodules commonly found on cheeks, nose, eyes) = pathognomonic for sarcoid and the most specific physical exam finding
Patient will present as →a 35-year-old female who was found to have a small (2.5 cm) pulmonary lesion on chest radiograph, found incidentally after a screening exam for a positive PPD at work. The patient has no significant past medical history and is asymptomatic.
Pulmonary nodules: < 3 cm = nodule; >3 cm = mass
Found on CXR ⇒ get CT
If suspicious ⇒ biopsy (ill-defined lobular or spiculated suggests cancer)
Not suspicious ⇒ < 1 cm monitor at 3 mo, 6 mo, then yearly for 2 yr (calcification, smooth well-defined edges = benign)
Radiographic characteristics help define the malignant potential of solitary pulmonary nodules
Growth rate determined by comparison of previous CXR or CT
The lesion that hasn’t grown in > 2 yr = benign
Double from 21-40 days = malignant
Small (< 1 cm) monitor at 3, 6, mo then yearly for 2 yr
Calcification suggests benign, especially if central, concentric popcorn
Margins that are spiculated or irregular ⇒ CA
Diameter < 1.5 cm strongly suggests benign; diameter > 5.3 cm strongly suggests CA



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}