Patient will present as →a 55-year-old female who is a non-smoker presents with a 9-month history of respiratory symptoms, including dyspnea on exertion, thoracic pain, and dry cough, which were preceded by a pulmonary infection. On auscultation, you hear inspiratory crackles. Pulmonary function tests (PFTs) show a restrictive pattern with a decreasein total lung capacity,decreased forced vital capacity (FVC), and preserved FEV1/FVC ratio.Chest CT demonstrates diffuse patchy fibrosis with pleural-based honeycombing.
Idiopathic pulmonary fibrosis (IPF) is a type of lung disease that results in scarring (fibrosis) of the lungs for an unknown reason
Over time, the scarring gets worse, and it becomes hard to take in a deep breath, and the lungs cannot take in enough oxygen
Etiology unknown; MC of all interstitial lung diseases
In order to be considered "idiopathic," you must rule out other common causes, such as drugs (amiodarone) and environmental or occupational exposures
non-idiopathic: smoking, viral infections, environmental (silica, hard metal dust), medication, genetics, XRT, GERD
Physical exam: Inspiratory crackles
DX: CXR shows fibrosis
CT chest: diffuse patchy fibrosis with pleural-based honeycombing
Decreased forced expiratory volume in the first second (FVC)
Decreased forced expiratory volume in the first second (FEV1)
Despite the reduction in FVC, the FEV1/FVC ratio is preserved or even increased because both FEV1 (forced expiratory volume in the first second) and forced vital capacity (FVC) are proportionally reduced
Tx: Few effective treatment options other than a lung transplant
Any fibrosis of the lung tissues with a known cause - usually from prolonged environmental or occupational contact
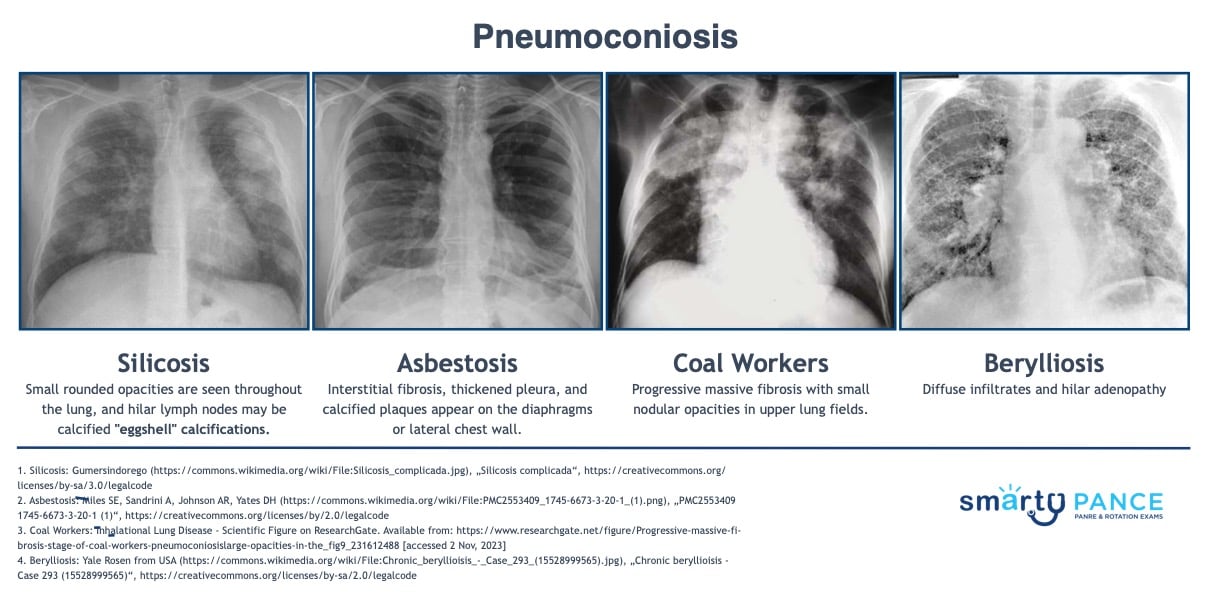
Patient with coal workers pneumoconiosis will present as → a 62-year-old male, a retired coal miner, who arrives at the clinic complaining of a persistent cough and shortness of breath that has gradually worsened over the past two years. He mentions he worked in coal mines for over 35 years. The cough is dry, and he denies any significant sputum production. He also reports a recent loss of appetite and mild weight loss. His medical history is significant for smoking a pack of cigarettes a day for 40 years, though he quit 5 years ago. On examination, he appears tachypneic with a respiratory rate of 22 breaths per minute. Auscultation of the lungs reveals bilateral rales but no wheezing. Chest X-ray shows small, rounded opacities throughout the lung fields and upper lobe predominance. Pulmonary function tests indicate a mild restrictive pattern.
Patient with silicosis will present as → a 57-year-old male working as a stone cutterwho comes to the clinic complaining of progressive breathlessness and a persistent dry cough over the last few months. He has been in the stone-cutting business for approximately 30 years and reports consistent exposure to dust without adequate respiratory protection. He denies smoking or any past significant medical history. On physical examination, he is noted to be short of breath while talking. Auscultation reveals fine bilateral end-inspiratory crackles, predominantly in the upper lobes. His oxygen saturation on room air is 94%. Chest X-ray demonstrates bilateral nodular opacities and hilar lymphadenopathy. High-resolution computed tomography (HRCT) of the chest confirms the presence of multiple small rounded nodules with upper lobe predominance and eggshell calcificationof the hilar nodes, supporting the diagnosis of silicosis.
Silicosis: mining, sandblasting, stone, quarry work; increased risk of TB and progression to massive fibrosis
CXR: small, rounded opacities throughout the lung, hilar lymph nodes may be calcified - "eggshell" calcifications
Patient with asbestosis will present as →a 53-year-old man presents to the office complaining of progressive dyspnea over the past few years. History reveals that he has worked in construction for the past 20 years, demolishing and refurbishing old buildings. He rarely uses any protective breathing equipment. Physical examination demonstrates an afebrile man in mild respiratory distress with inspiratory crackles. The chest x-ray reveals a reticular linear pattern with basilar predominance, opacities, and honeycombing.
CXR: interstitial fibrosis, thickened pleura, calcified plaques appear on diaphragms or lateral chest wall
Patient with Berylliosis will present as → a 52-year-old female who works in an aerospace manufacturing facility, presenting with a 6-month history of increasing shortness of breath, dry cough, and fatigue. She reports no smoking history or significant past medical issues. On examination, she appears to be in respiratory distress, with a respiratory rate of 26 breaths per minute. Auscultation of her lungs reveals diffuse crackles. Chest X-ray shows bilateral infiltrates and hilar lymphadenopathy. Her work history reveals prolonged exposure to beryllium. Pulmonary function tests indicate a restrictive pattern and a subsequent lung biopsy demonstrates noncaseating granulomas. A beryllium lymphocyte proliferation test (BeLPT) confirms the diagnosis of chronic berylliosis.
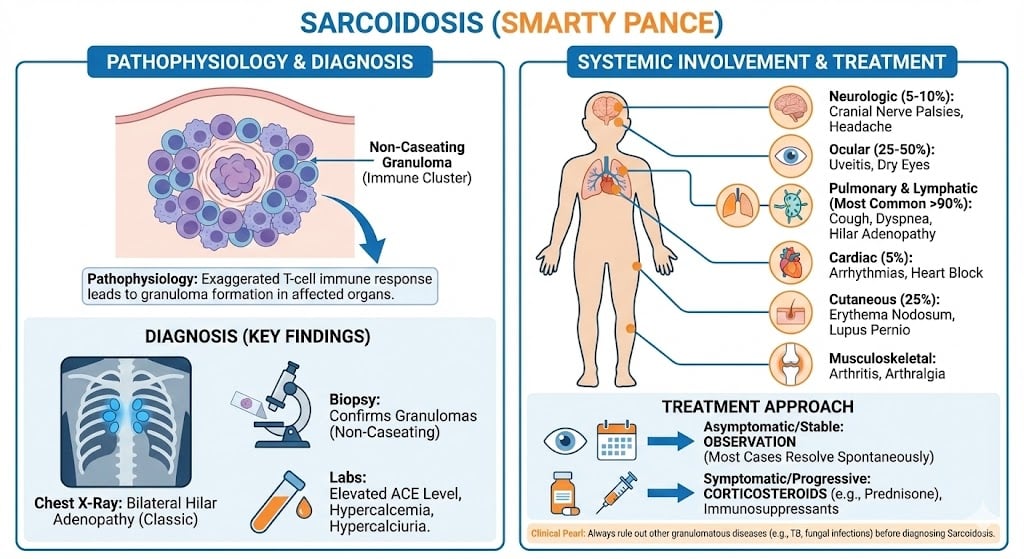
Patient will present as → a 38-year-old African-American woman who visits the clinic complaining of persistent dry cough, shortness of breath, and mild chest pain for the past two months. She also notes occasional fevers and unexplained weight loss. You note erythema nodosum on her lower legs. Her chest X-ray reveals bilateral hilar lymphadenopathy and reticular opacities. Pulmonary function tests show a restrictive lung disease pattern. Laboratory findings include elevated serum angiotensin-converting enzyme (ACE) levels. A biopsy of the lymph nodes obtained during bronchoscopy demonstrates noncaseating granulomas, consistent with a diagnosis of sarcoidosis.
Chronic autoimmune inflammatory disease in which small nodules (granulomas) develop in lungs, lymph nodes, and other organs
Lupus pernio (chronic, violaceous, raised plaques and nodules commonly found on cheeks, nose, eyes) = pathognomonic for sarcoid and most specific physical exam finding
DX: Sarcoidosis is diagnosed by compatible clinical and radiographic findings with biopsy-proven noncaseating granulomas after excluding infection and malignancy
Biopsy → non-caseating granulomas
"Sarcoidosis causes elevated ACE and hypercalcemia because activated macrophages within granulomas produce ACE and convert inactive vitamin D into its active form, increasing intestinal calcium absorption."
TX: Steroids = 90% respond to steroid
Methotrexate, other immunosuppressive meds
Serial PFTs to assess disease progression/guide treatment
ACE-I for periodic HTN
Prognosis depends on disease severity; spontaneous improvement common
 Osmosis
Osmosis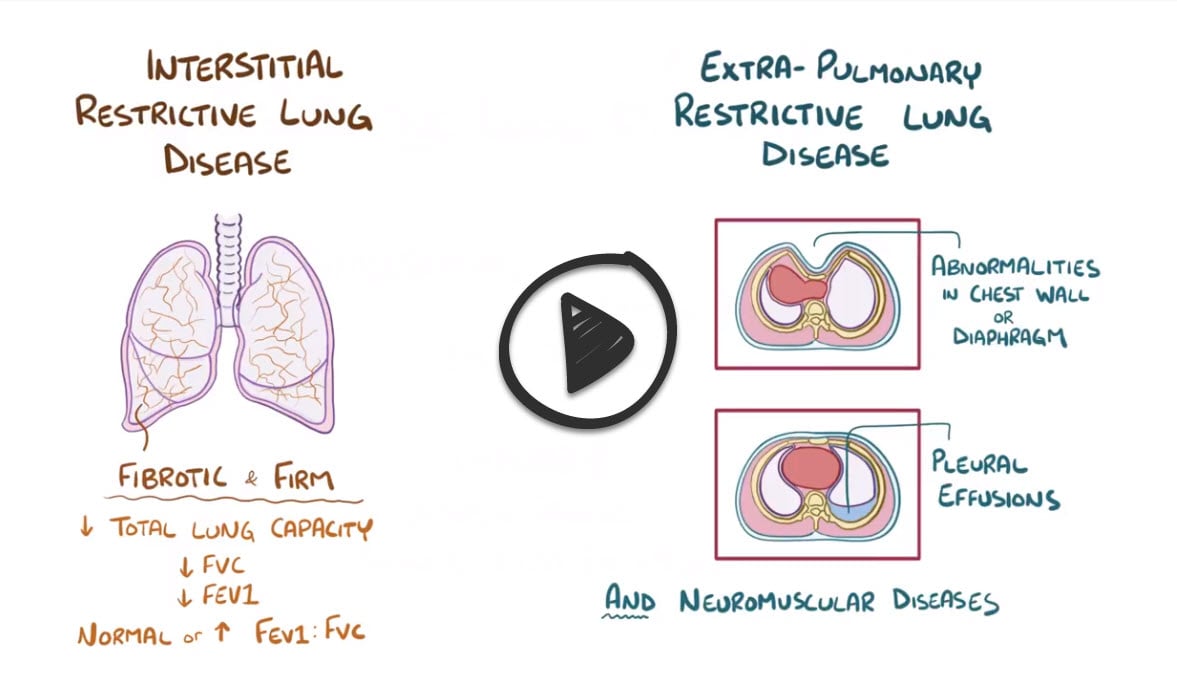




{kind=link}