
Patient will present as → a 67-year-old male with a 6-month history of progressive shortness of breath on exertion and a persistent dry cough. He has a past medical history of hypertension, controlled with medication, and a 30-pack-year smoking history, although he quit smoking 10 years ago. He denies any significant occupational exposures or a family history of lung disease. On examination, he appears tachypneic with a respiratory rate of 22 breaths per minute. Auscultation of the lungs reveals bilateral fine inspiratory crackles at the lung bases. His oxygen saturation on room air is 92%. Pulmonary function tests show a restrictive pattern with reduced forced vital capacity (FVC) and a preserved FEV1/FVC ratio. Diffusion capacity for carbon monoxide (DLCO) is significantly reduced. High-resolution computed tomography (HRCT) of the chest demonstrates bilateral reticular opacities, honeycombing, and traction bronchiectasis predominantly at the lung bases, without significant lymphadenopathy or pleural effusion. A diagnosis of Idiopathic Pulmonary Fibrosis is made. The patient is counseled about the nature of the disease, including its progressive course and the current lack of a cure. Treatment options, including antifibrotic therapy with nintedanib or pirfenidone to slow disease progression, are discussed. The importance of pulmonary rehabilitation, vaccinations, and supplemental oxygen therapy as needed is emphasized. The patient is also advised on lifestyle modifications, including regular exercise and smoking cessation support for his prior smoking habit. Referrals to a support group for patients with IPF and a palliative care consultation to manage symptoms and improve quality of life are provided.
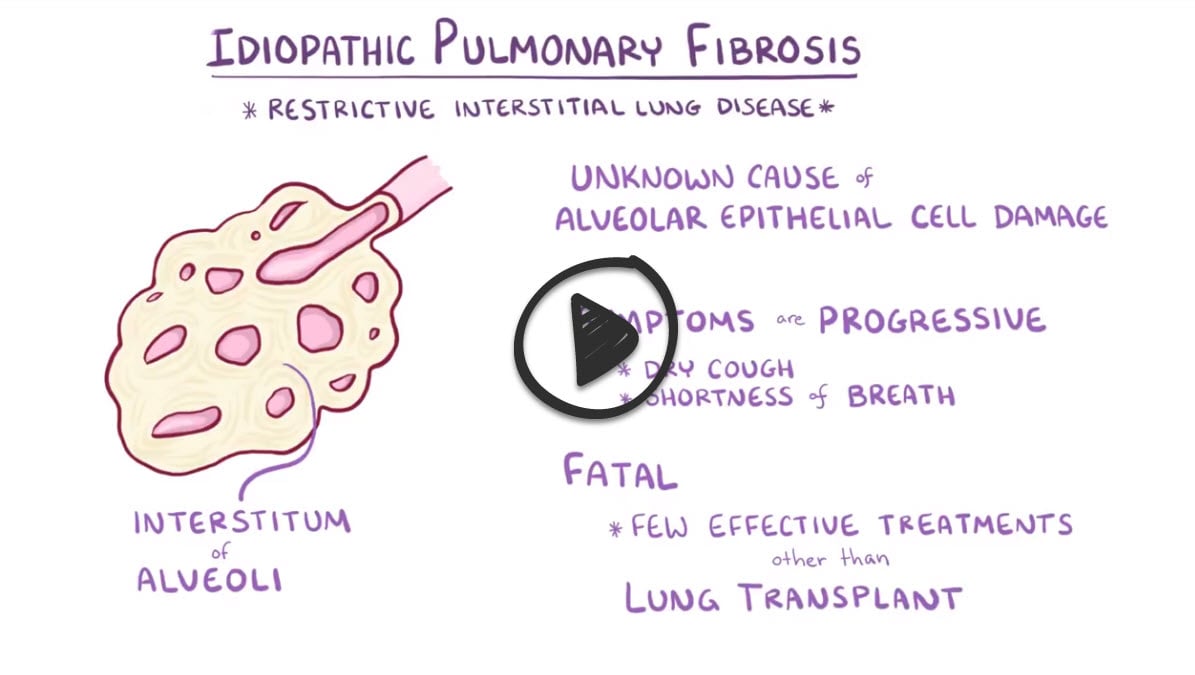
Chronic progressive lung disorder characterized by increasing scarring, which ultimately reduces the capacity of the lungs; etiology unknown
- Idiopathic pulmonary fibrosis is the most common of all interstitial lung diseases
- In order to be considered "idiopathic," you must be sure to rule out other common causes, such as drugs and environmental or occupational exposures
Common "non-idiopathic" causes of pulmonary fibrosis which must be ruled out:
- Cigarette smoking
- Certain viral infections
- Exposure to environmental pollutants, including silica and hard metal dusts, bacteria and animal proteins, and gases and fumes
- The use of certain medicines (methotrexate, amiodarone, nitrofurantoin, rituximab, bleomycin, and cyclophosphamide)
- Genetics
- Radiation treatment
- Gastroesophageal reflux disease (GERD)
CXR shows fibrosis
- CT chest: diffuse patchy fibrosis with pleural-based honeycombing
- PFTs will demonstrate a restrictive pattern - the opposite of what you would see with asthma
- Decreased total lung capacity, decreased forced vital capacity (FVC), decreased forced expiratory volume in one second (FEV1)
- The FEV1/FVC ratio may be normal or greater than 80% (increased) due to a significant decrease in forced vital capacity (FVC)
- Despite the reduction in FVC, the FEV1/FVC ratio is preserved or even greater than 80% (increased) because both FEV1 (forced expiratory volume in the first second) and forced vital capacity (FVC) are proportionally reduced

Pulmonary fibrosis induced by amiodarone.

Chest CT showing classic “honeycombing”
Treatment may include antifibrotic drugs (pirfenidone or nintedanib), oxygen therapy, and eventually lung transplant
- Most patients deteriorate, and the median survival is about 3 years from diagnosis
 Osmosis Osmosis |
|
 |
Restrictive lung diseases can be caused by either poor breathing mechanics, a result of conditions like myasthenia gravis, obesity, and scoliosis. They can also result from interstitial lung disease such as pneumoconioses or ARDS. Lung volume decreases in restrictive lung disease and the FEV1/FVC ratio is greater than 80% due to a significant decrease in forced vital capacity (FVC). FEV1 is the forced expiratory volume in 1 second or the volume of air that can forcibly be blown out in one second, after full inspiration. FVC is the forced vital capacity or the volume of air that can forcibly be blown out after full inspiration. Both these values can be measured by spirometry. The ratio between the FEV1 and FVC can help distinguish between restrictive and obstructive lung diseases. A ratio greater than 80% suggests a restrictive condition.
Play Video + QuizObstructive lung disease

Obstructive lung disease is characterized by airway obstruction and it is associated with inflammation of the airways and problems exhaling. Types of obstructive lung disease are asthma, bronchiectasis, bronchitis, and COPD. Obstructive lung disease results in air trapping in the lungs which expands the lung volume over time. A decrease in FEV1/FVC ratio suggests an obstructive condition.
Play Video + QuizRestrictive vs. Obstructive Lung Diseases

Lung diseases can be classified as either restrictive or obstructive. Restrictive lung diseases cause a decrease in lung volume. Obstructive lung diseases trap air in the lungs and therefore increase lung volume.
Play Video + QuizQuestion 1 |
Early inspiratory crackles Hint: Late, not early, inspiratory crackles are associated with interstitial lung disease. | |
Progressive dyspnea on exertion | |
Productive cough with copious sputum Hint: A productive cough of copious amounts of sputum is most typical of a patient with chronic bronchitis. | |
Decreased breath sounds with hyperresonant percussion Hint: Physical examination findings of decreased breath sounds with hyperresonant percussion is consistent with a diagnosis of chronic obstructive lung disease. |
Question 2 |
COPD Hint: COPD appears as hyperinflation with flattening of the diaphragm on chest radiograph | |
Tuberculosis Hint: Tuberculosis presents with pulmonary infiltrates on chest radiograph most often apical; cavitations may be seen with progressive primary tuberculosis. | |
Bronchiectasis Hint: Chest x-ray in bronchiectasis shows dilated and thickened bronchi that appear as ring-like markings. | |
Pulmonary fibrosis |
|
List |
References: Merck Manual · UpToDate