The NCCPA™ PANCE and PANRE Pulmonary Content Blueprint requires you to understand and differentiate between 4 types of infectious pneumonia
| Bacterial pneumonia (ReelDx) | Patient will present as → a 40-year-old alcoholic male with sudden onset of severe chills, fever, dyspnea, and cough productive of red mucoid sticky sputum. He appears ill-looking with cyanosis. Examination reveals vital signs: Temp – 102 degrees F; Pulse – 120 /minute and regular; 89 RR – 28/min; BP 90/62 mm Hg. Lungs reveal minimal rales and dullness in the right upper lobe with decreased breath sounds. Chest x-ray reveals right upper lobe consolidation with a bulging fissure. Gram stain reveals many white blood cells and many gram-negative rods. (klebsiella pneumoniae) Common Pathogens and Key Clues
DX: Requires both:
 A chest X-ray showing a very prominent wedge-shaped area of airspace consolidation in the right lung, characteristic of bacterial pneumonia. TX: Risk-stratify CAP using CURB-65 or PSI) to determine outpatient vs inpatient management
|
| Viral pneumonia | Patient will present as → a 45-year-old male with a one-week history of hacking, non-productive cough, low-grade fever, malaise, and myalgias. The chest x-ray reveals bilateral interstitial infiltrates and a cold agglutinin titer that is negative. Examination reveals scattered rhonchi and rales upon auscultation of the chest. Adults → The influenza viruses are the most common viral cause of pneumonia
Kids → RSV, 1st episode of wheezing
Parainfluenza virus pneumonia
DX: Chest radiography usually demonstrates bilateral lung involvement, but none of the viral etiologies of pneumonia result in pathognomonic findings with CXR
TX: Influenza can be treated with oseltamivir (Tamiflu)
RSV pneumonia
PIV pneumonia
 Chest radiograph from a patient with viral pneumonia showing widespread bilateral interstitial infiltrates |
| Fungal pneumonia | Patient with valley fever will present as → a 38-year-old construction worker who recently moved to Phoenix, Arizona, for a new project. Over the past two weeks, he’s been experiencing fatigue, cough, and intermittent fevers. He also mentions having chest pain that worsens when he takes a deep breath. He recalls a dusty wind storm at the construction site about three weeks ago. On physical examination, you note a few erythematous, tender nodules on his shins. Chest radiography shows a nodular pattern in the right lung field. Given his symptoms and exposure history, a sputum sample is sent for fungal cultures. Coccidioides (valley fever): Look for this in a patient with non-remitting cough/bronchitis non-responsive to conventional treatments.
Patient with Histoplasmosis will present with → a 21-year-old male presents with a cough and mild shortness of breath for three days. The cough is productive of yellowish mucus. He reports a low-grade fever with this episode but says that he has otherwise been healthy. He has spent the last month working in bat caves. He denies tobacco or alcohol use. Histoplasma capsulatum is an opportunistic fungus that is known to cause systemic disease in HIV patients that involves low-grade fevers, cough, hepatosplenomegaly, and tongue ulceration
 Chest film showing diffuse pulmonary infiltration and hilar lymphadenopathy due to acute pulmonary histoplasmosis. Patient with Cryptococcus will present as → a 49-year-old HIV-positive male with a CD4 count of 9. He lives alone and drinks daily. He presents to the hospital with a headache, neck stiffness, and confusion. A lumbar puncture (LP) shows that his intracranial pressure is very high (45 cm) and that his spinal fluid contains Cryptococcus (India Ink and CrAg positive). Baseline blood ordered: full blood count, creatinine, ALT, and RPR. The serum cryptococcal antigen (CrAg) test is positive. Cryptococcus: Caused by the fungus Cryptococcus neoformans, common in AIDS and immunocompromised states, is considered an AIDS-defining illness
Pulmonary aspergillosis: The majority of cases occur in people with underlying illnesses such as tuberculosis or chronic obstructive pulmonary disease (COPD), but with otherwise healthy immune systems
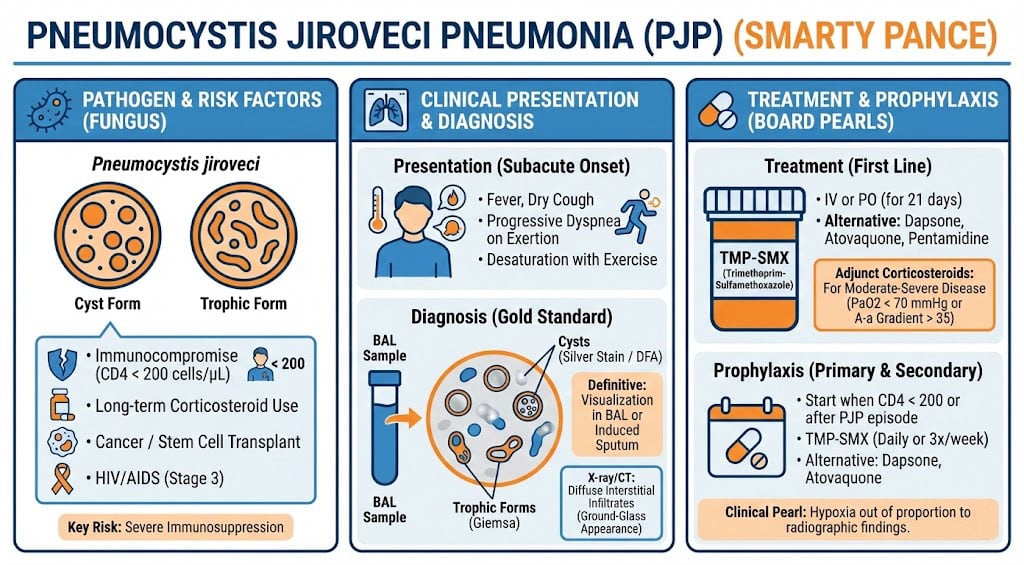
Patient with PJP Pneumonia will present as → a 32-year-old man with a two-week history of fever and dry, nonproductive cough. For the past five days, he has been having shortness of breath. There is no history of pleuritic chest pain or rigors.Past medical history is significant for HIV. His temperature is 100.4°F (38°C), pulse is 92/min, O2 saturation is 92%, respirations are 18/min, and blood pressure is 120/70 mmHg. Purified protein derivative (PPD) is negative. CD4 cell count is 190. The chest exam reveals bibasal crackles. The chest radiograph shows interstitial infiltrates bilaterally. The patient’s condition worsens on levofloxacin. Pneumocystis Jiroveci (formerly PCP Pneumonia, now called PJP)
|
| HIV-related pneumonia | Patient will present as → a 32-year-old HIV+ male with dyspnea and a nonproductive cough. He is tachycardic, tachypneic and febrile. Auscultation of his chest reveals scattered rhonchi. His chest x-ray demonstrates a diffuse interstitial infiltrate. His ABG demonstrates moderate hypoxemia, and his LDH is elevated
Formerly PCP Pneumonia, now called (PJP) Pneumocystis jiroveci (there are other HIV-related types of pneumonia, but this is the one you will need to know for the test)
DX: CXR is the cornerstone of diagnosis. The radiograph shows diffuse interstitial OR bilateral perihilar infiltrates
TX: Trimethoprim-sulfamethoxazole (Bactrim) and steroids
Prophylaxis for high-risk patients with a CD4 count of less than 200 or with a history of PJP infection
 These chest radiographs are of two patients. Both show a ground-glass appearance. The left chest X-ray (CXR) shows a much more subtle ground-glass appearance, while the right CXR shows a much more gross ground-glass appearance mimicking pulmonary edema. |