The NCCPA™ PANCE Pulmonary Content Blueprint: obstructive pulmonary diseases
| Asthma (ReelDx) | Patient will present as → a 22-year-old female presents with intermittent wheezing and dyspnea triggered by exercise and cold air, occurring about twice monthly. She denies nighttime symptoms or prior exacerbations. Physical exam and spirometry are normal; bronchodilator testing confirms reversible obstruction. She is diagnosed with asthma (GINA Step 1) and started on as-needed low-dose ICS–formoterol. She receives education on trigger avoidance and inhaler technique and is given an asthma action plan. Follow-up is planned in 6–8 weeks. ReelDx Virtual Rounds (asthma)Asthma is a chronic, reversible inflammatory airway disease characterized by episodic bronchoconstriction, airway hyperresponsiveness, and mucus production
Diagnosis and Monitoring
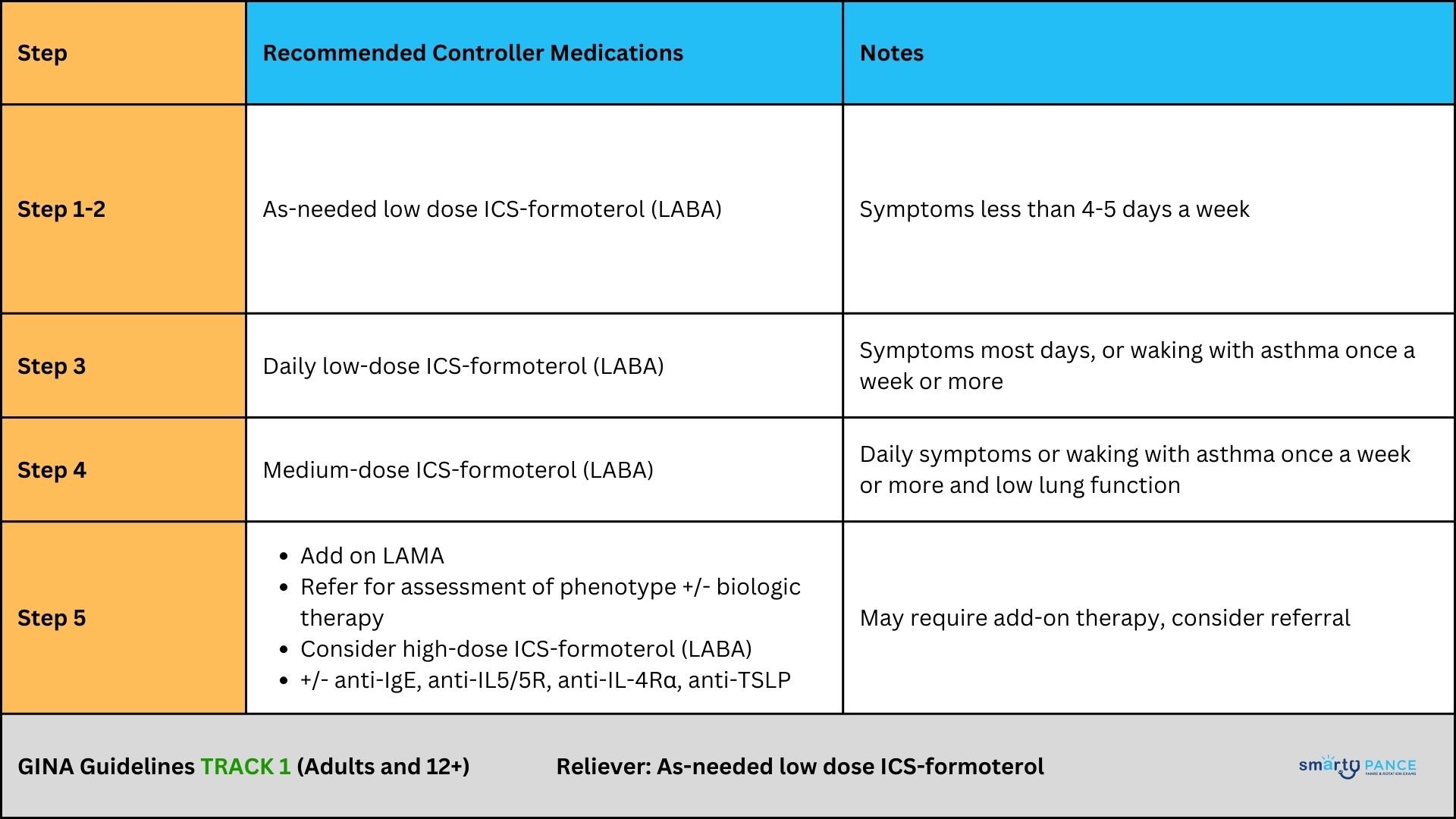
Treatment Guidelines Previously, asthma was labeled 'mild intermittent' or 'severe persistent,' but GINA now recommends a treatment-based approach (Step 1–5) based on both symptom control and exacerbation risk. The Global Initiative for Asthma (GINA) strategy divides asthma treatment into two tracks for adults and adolescents:
Table 1: GINA Track 1
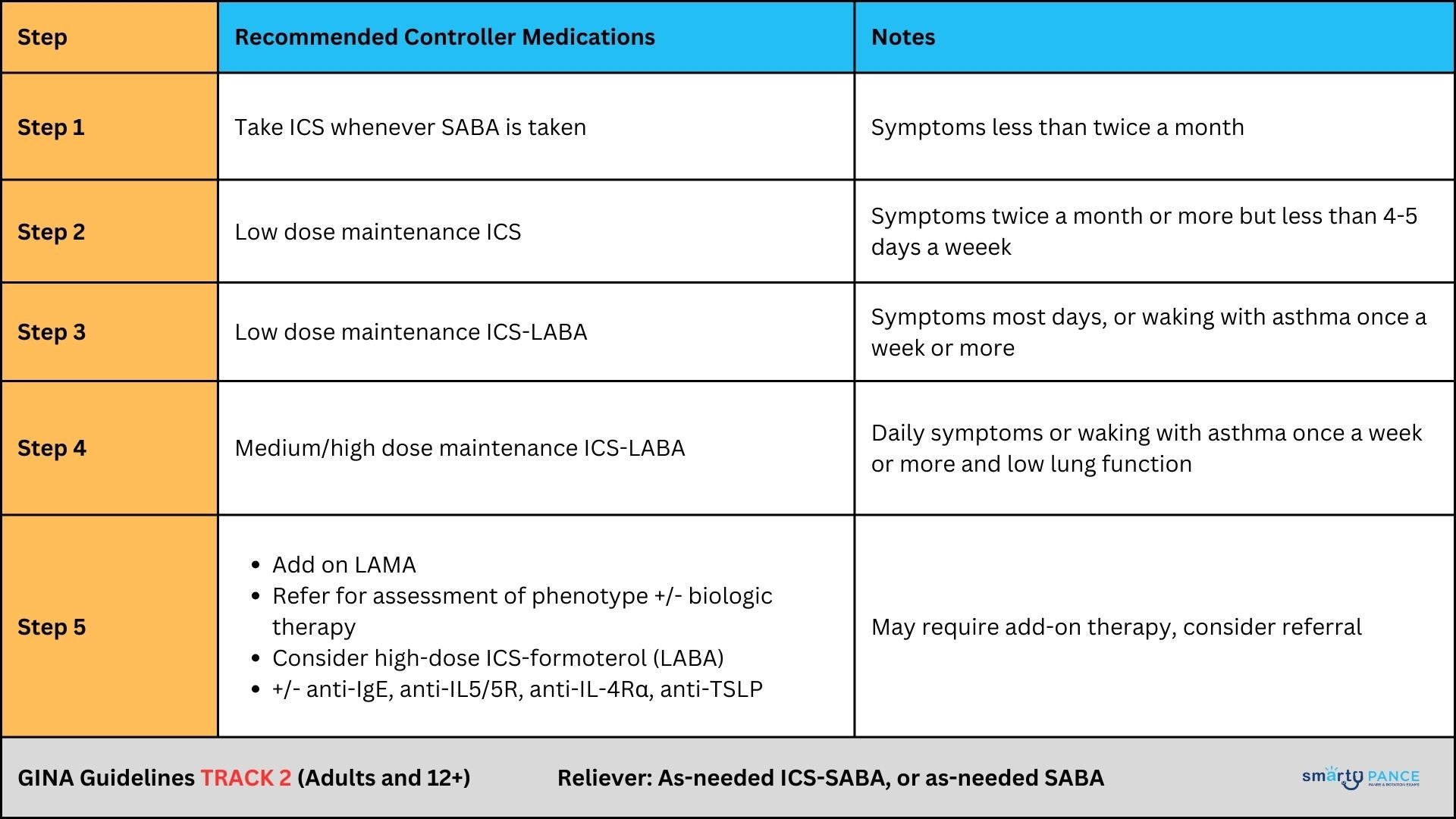
Table 2: GINA Track 2
Acute Treatment
Dosing for GINA Tracks (Adolescents and Adults ≥12 Years)
Pricing (Approximate, U.S. Market, 120-dose inhaler) Symbicort (budesonide/formoterol, available as metered-dose inhaler [MDI] or dry powder inhaler [DPI/Turbuhaler])
Track 1: ICS-Formoterol as Maintenance and Reliever (SMART)
Track 2: ICS/LABA Maintenance with SABA Reliever
Making Sense of Forced Vital Capacity
|

|
Chronic obstructive pulmonary disease Chronic Obstructive Pulmonary Disease (COPD) is a progressive, irreversible airway disease characterized by airflow limitation due to chronic bronchitis, emphysema, or both Chronic bronchitis is defined by clinical features (chronic cough) vs. emphysema, which is characterized by structural changes (enlarged air spaces secondary to alveolar destruction) |
|
| Chronic Bronchitis | Emphysema |
| A type of COPD marked by a chronic, mucus-producing cough lasting at least 3 months per year for 2 or more years, not due to another apparent cause. | A form of COPD characterized by enlargement of air spaces and destruction of alveolar septae, often resulting in a barrel-chested appearance. |
|
|

Obstructive lung disease is characterized by airway obstruction and associated with inflammation of the airways. Air trapping as a result of airway obstruction causes an increase in the residual volume of the lungs, which means the volume of air left in the lungs after fully exhaling is increased. Forced vital capacity, the volume of air that can be forcibly blown out after one full inspiration, is decreased. FEV1, the forced expiratory volume in 1 second or the volume of air that can be forcibly blown out in 1 second, is also decreased. More importantly, the ratio of FEV1/FVC is decreased because even though FVC is decreased, the FEV1 decreases even greater resulting in an overall decrease in the FEV1/FVC ratio. This can be clearly distinguished from restrictive lung disease which has a ratio greater than 80%. Common obstructive lung diseases include chronic bronchitis, emphysema, asthma, and bronchiectasis.
Play Video + Quiz| Chronic bronchitis | Patient will present as → a 56-year-old female with shortness of breath and a productive cough that has occurred over the past two years for at least three months each year. She is a heavy smoker. Physical exam reveals a respiratory rate of 32, slightly labored breathing, and a temperature of 98.9°F. Her SpO2 is 90% while receiving oxygen via nasal cannula at 2 LPM. Chronic bronchitis is defined as a chronic cough that is productive of phlegm occurring on most days for 3 months of the year for two or more consecutive years without an otherwise defined acute cause
 "The common organisms causing pneumonia in patients with COPD are Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis. Patients who smoke are often colonized with Haemophilus influenza." DX: Board bottom line: spirometry makes the diagnosis — a post-bronchodilator FEV1/FVC <0.70 — and GOLD 1–4 grades how severe.
TX: Board pearl: only smoking cessation and long-term oxygen reduce mortality — everything else treats symptoms and exacerbations.
GOLD A / B / E groups — initial maintenance therapy
 Chest X-ray of chronic bronchitis showing increased bronchial markings and perivascular haziness from airway inflammation. |
||||||||||||
| Emphysema | Patient with emphysema will present as → a 65-year-old male complaining of fatigue and shortness of breath with exertion. The patient reports minimal cough. On physical exam, you note a thin, barrel-chested man with decreased heart and breath sounds, pursed-lip breathing, end-expiratory wheezing, and scattered rhonchi. Chest X-ray reveals a flattened diaphragm, hyperinflation, and a small, thin-appearing heart. PFTs show a decreased FEV1/FVC ratio. Emphysema is a condition in which air spaces are enlarged due to destruction of the alveolar septa
DX:
TX: Management is the same as Chronic Bronchitis
 Chest X-ray of bullous emphysema showing large bullae (air pockets from alveolar destruction) (arrow), hyperinflation, reduced lung markings, a small, thin appearing heart, and a flattened diaphragm. |
||||||||||||
| Cystic fibrosis | Patient will present as → a 7-year-old boy brought by his parents due to a persistent cough, wheezing, and recurrent lung infections since infancy. The parents also report the child having bulky, foul-smelling stools and difficulty gaining weight despite a good appetite. On exam, he appears underweight with digital clubbing. Sweat chloride test shows 88 mmol/L. The stool elastase test is low. Genetic testing confirms CFTR mutations. Management includes airway clearance, enzyme replacement, a high-calorie diet, and referral to a CF center. Cystic fibrosis (CF) affects secretions — they become thick and sticky → block airways and ducts
Presentation:
DX:
TX:
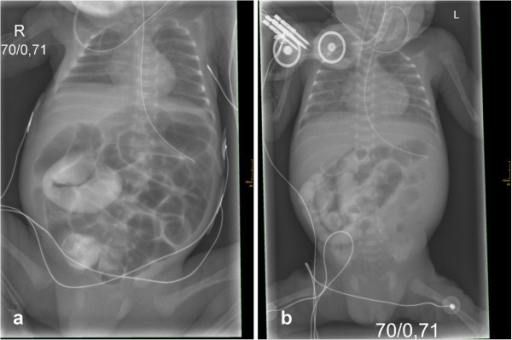 Meconium ileus in preterm twins revealing a novel cystic fibrosis mutation. Image by Department of Pediatrics, Albert-Ludwigs-University of Freiburg, Mathildenstrasse 1, D 79106 Freiburg, Germany. [email protected]. License: CC BY 2.0 |