 Osmosis
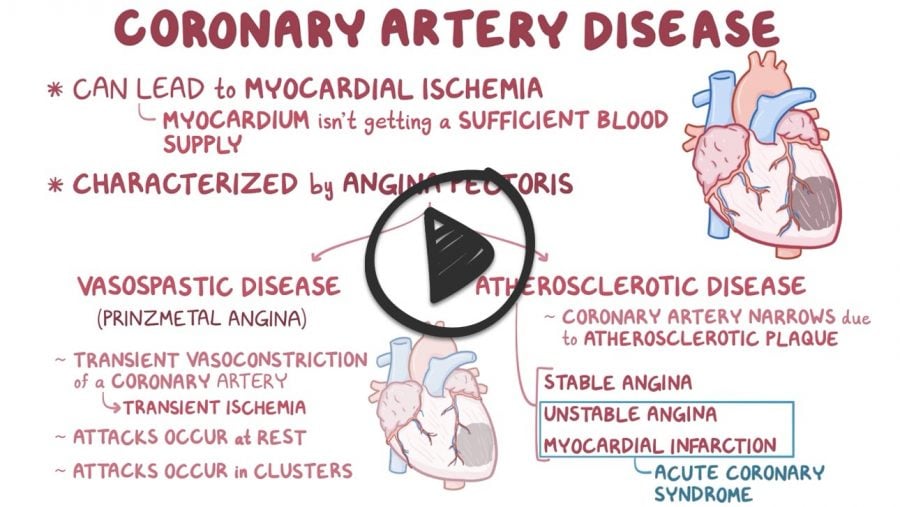
Osmosis| Stable angina | Chest pain or discomfort, heaviness, pressure, squeezing, tightness that is increased with exertion or emotion
Workup:
Treatment:
Prognosis:
|
| Unstable angina | Chest pain or discomfort, heaviness, pressure, squeezing, tightness that is increased with exertion or emotion
Workup:
Treatment
|
| Prinzmetal variant angina | Coronary artery vasospasms causing transient ST-segment elevations, not associated with clot
Nonexertional chest pain similar to unstable angina
Diagnostics:
Treatment:
|
Congratulations - you have completed Unsable Angina.
You scored %%SCORE%% out of %%TOTAL%%.
Your performance has been rated as %%RATING%%
Your answers are highlighted below.
Question 1 |
A 55 year-old male is seen in follow-up for a complaint of chest pain. Patient states that he has had this chest pain for about one year now. The patient further states that the pain is retrosternal with radiation to the jaw. "It feels as though a tightness, or heaviness is on and around my chest". This pain seems to come on with exertion however, over the past two weeks he has noticed that he has episodes while at rest. If the patient remains inactive the pain usually resolves in 15-20 minutes. Patient has a 60-pack year smoking history and drinks a martini daily at lunch. Patient appears overweight on inspection. Based upon this history what is the most likely diagnosis?
Acute myocardial infarction Hint: Pain does not resolve in an acute MI, it gradually gets worse. | |
Prinzmetal variant angina Hint: Pain typically occurs at rest is one of the hallmarks of Prinzmetal variant angina. This patient has just started to develop pain at rest. | |
Stable angina Hint: Pain in stable angina is relieved with rest and usually resolves within 10 minutes. angina does not have pain at rest. | |
Unstable angina |
Question 1 Explanation:
Pain in unstable angina is precipitated by less effort than before or occurs at rest.
Question 2 |
A 58 year-old male who is otherwise healthy presents with chest pain and is found to have left main coronary artery stenosis of 75%. The most important aspect of his management now is
daily aspirin to prevent MI. Hint: See D for explanation. | |
nitrate therapy for the angina. Hint: See D for explanation. | |
aggressive risk factor reduction. Hint: See D for explanation. | |
referral for coronary artery revascularization. |
Question 2 Explanation:
Although medical therapy is important, revascularization is indicated when stenosis of the left main coronary artery is greater than 50%.
Question 3 |
A 60 year-old male with history of hypertension and hyperlipidemia presents with intermittent chest heaviness for one month. The patient states he has had occasional heaviness in his chest while walking on his treadmill at home or shoveling snow. He also admits to mild dyspnea on exertion. His symptoms are relieved with 2-3 minutes of rest. He denies lightheadedness, syncope, orthopnea or lower extremity edema. Vitals reveal a BP of 130/90, HR 70, regular, RR 14. Cardiac examination revealed a normal S1 and S2, without murmur or rub. Lungs were clear to auscultation. Extremities are without edema. EKG reveals no acute change and cardiac enzymes are negative. Which of the following is the most appropriate next diagnostic study?
cardiac catheterization Hint: Coronary angiography is indicated in patients with classic stable angina who are severely symptomatic despite medical therapy and are being considered for percutaneous intervention (PCI), patients with troublesome symptoms that are difficult to diagnose, angina symptoms in a patient who has survived sudden cardiac death event, patients with ischemia on noninvasive testings, a stress test is a better initial diagnostic study for this patient. | |
nuclear exercise stress test | |
helical (spiral) CT Hint: Helical CT is used in the diagnosis of pulmonary embolism, not in the evaluation of angina. | |
transthoracic Echocardiogram Hint: Echocardiogram is used in the evaluation of valvular heart disease not in the evaluation of suspected myocardial ischemia. |
Question 3 Explanation:
This patient has signs and symptoms of classic angina; nuclear stress testing is the most useful noninvasive procedure for diagnosis of ischemic heart disease and evaluation of angina in this patient.
Once you are finished, click the button below. Any items you have not completed will be marked incorrect.
There are 3 questions to complete.
|
List |