


37 y/o with left lower leg swelling and pain, left-sided chest pain, and SOB
Patient will present as → a 78-year-old female complaining of generalized pain and edema in her left leg. She denies chest pain, shortness of breath, and hemoptysis. She takes 2.5 mg warfarin daily for atrial fibrillation and her INR is 2.6. On physical examination the patient experience calf pain with dorsiflexion of the left foot. The patient has a positive D-dimer and a lower extremity ultrasound reveals the presence of a deep venous thrombosis in the left popliteal vein.
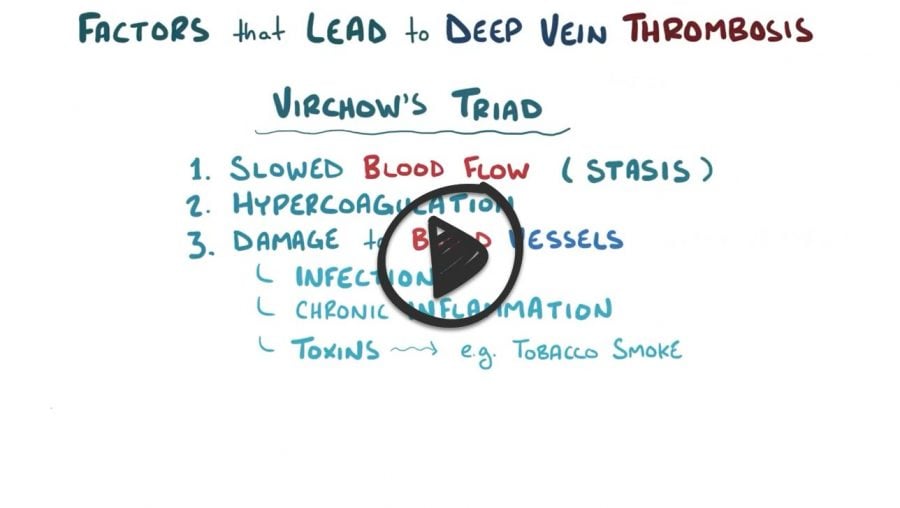
Caused by a clot formation in the veins. Virchow's triad determines risk factors for clot formation.
- Stasis: post-surgical, immobility, venous insufficiency.
- Hypercoagulable states: Factor V Leiden, cancer, OCP + smoking, pregnancy.
- Trauma: surgery, cellulitis.
Will present with edema of one extremity, and a positive Homan's sign (extend leg and push the foot towards the head with pain in the calf)
*Women over age 35 who smoke are at increased risk for the development of venous thrombosis and women older than 35 years who smoke should avoid oral contraceptive pills. Progestin-Only hormonal methods are a reasonable alternative in this population.
Venous duplex ultrasound is first line imaging test
- D-dimer - a negative D-dimer will rule out DVT in low-risk patients
- Venography is considered GOLD STANDARD
Treat with IV heparin and switch to Warfarin
- Recurrent DVT requires lifetime anticoagulation
Adapted from surgical recall, by Lorne Blackbourne
 Osmosis Osmosis |
|
 |

Deep vein thrombosis (DVT) is a venous thromboembolism (VTE) that is often asymptomatic with clinical signs that are nebulous, including a combination of swelling, pain, and warmth. Diagnostic tests then become of utmost importance in determining the proper course of action. Diagnosis can be supported or accomplished via a variety of studies, including compression ultrasound (CUS) with doppler, D-dimer, and contrast venography. Treatment is dependent on a variety of factors, but options include heavy-hitting therapies such as an inferior vena cava (IVC) filter, heparin, warfarin, and thrombectomy/thrombolysis in addition to less aggressive, preventative measures such as compression stockings and walking.
Play Video + QuizDeep Vein Thrombosis (DVT) Characteristics
Deep vein thrombosis (DVT) is a serious complication in patients with specific risk factors. Patients who fulfill any part of Virchow’s triad may develop DVT, which presents as redness, swelling, warmth, tenderness, and a positive Homan’s sign. Often, patients can be asymptomatic.
Question 1 |
venous thrombosis. | |
varicose veins. Hint: Varicose veins are the result of pressure overload on incompetent veins and not due to the use of oral contraceptives. | |
atherosclerosis. Hint: The defined risks of atherosclerosis includes smoking, but does not include the use of oral contraceptives. | |
peripheral edema. Hint: There is no relationship between the use of oral contraceptives and the development of peripheral edema. |
Question 2 |
Venogram Hint: Venogram has been replaced by noninvasive tests due to discomfort, cost, technical difficulties, and complications, such as phlebitis. | |
Arteriogram Hint: Thrombophlebitis is a venous problem, not an arterial one. Any unnecessary invasive procedure is potentially harmful. | |
Duplex ultrasound | |
Impedance plethysmography Hint: Impedance plethysmography is equivalent to ultrasound in detecting thrombi of the femoral and popliteal veins, but it may miss early, nonocclusive thrombi. |
Question 3 |
Admission for intravenous unfractionated heparin (UFH) Hint: IV UFH is generally reserved for patients with severe DVT, those with high bleeding risk, or if rapid anticoagulation reversal might be needed. | |
Inferior vena cava (IVC) filter placement Hint: While IVC filters can prevent pulmonary emboli, they are primarily indicated in patients with DVT who can't tolerate anticoagulation, not as the initial treatment. | |
Initiation of a direct oral anticoagulant (DOAC) | |
Thrombolytic therapy with alteplase Hint: Thrombolysis is reserved for high-risk, extensive DVTs or those causing limb-threatening ischemia. It carries a higher bleeding risk compared to standard anticoagulation. | |
Warfarin with heparin bridging Hint: This was the traditional approach but now superseded by DOACs, which don't require bridging therapy and offer simpler management. |
|
List |