
Patient will present as → a 75-year-old male with a history of hypertension and mild cognitive impairment presents to the emergency department following a fall at home two days ago. He reports hitting his head on the ground but did not lose consciousness. Since the fall, his family has noticed that he has become increasingly confused and lethargic. He also complains of a persistent headache. On examination, he is oriented to person but not to time or place. His pupils are equal and reactive, but he has a mild weakness in his right arm and leg. A CT scan of the head reveals a crescent-shaped hyperdense collection over the left cerebral hemisphere, consistent with an acute subdural hematoma. There is a midline shift indicating increased intracranial pressure. The patient is admitted to the neurosurgical unit, and an urgent neurosurgical consultation is obtained. He undergoes a craniotomy for evacuation of the hematoma. Postoperatively, he is monitored in the intensive care unit. His postoperative course includes gradual improvement in his mental status and motor strength. He is referred to physical and occupational therapy for rehabilitation and scheduled for follow-up appointments to monitor his recovery.
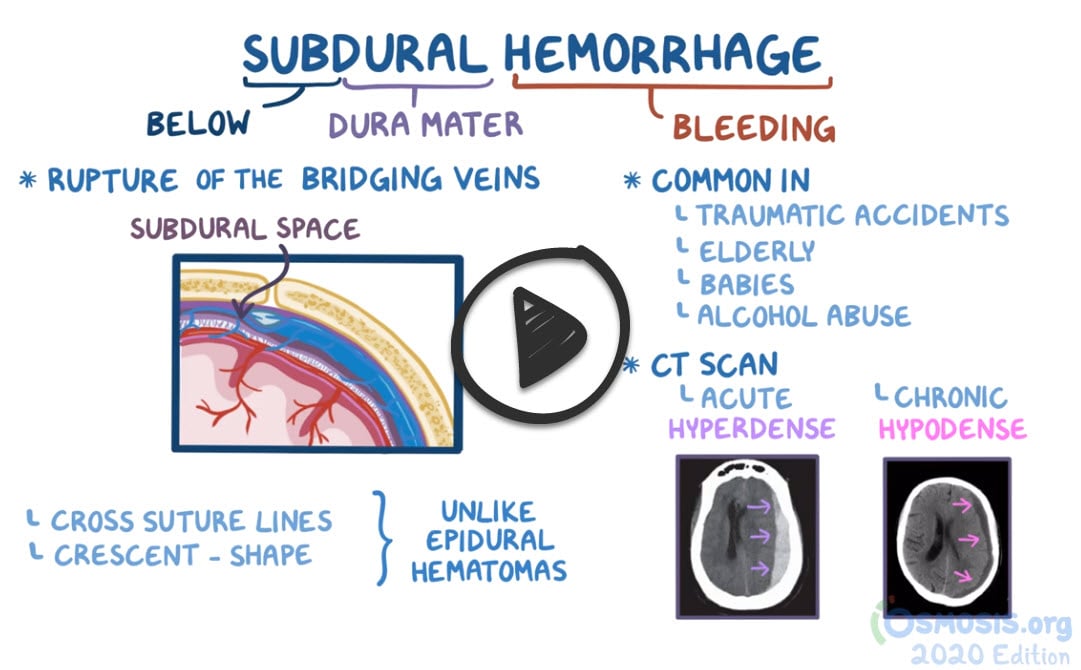
Subdural hematoma is usually caused by a head injury, such as from a fall, motor vehicle collision, or assault. The sudden blow to the head tears blood vessels that run along the surface of the brain.
- The likely scenario is an elderly patient with a history of multiple falls who is now presenting with neurological symptoms – indicative of a chronic subdural hematoma.
- Subdural hematomas usually result from injuries to bridging veins.
- Acute: symptoms within 48 hours of injury.
- Subacute: symptoms within 3 to 14 days.
- Chronic: symptoms after 2 weeks or longer - common in alcoholics and elderly patients.
- A subdural hematoma can occur after an apparently minor trauma and is associated with mental status changes or focal neurologic signs.
CT is diagnostic; once the diagnosis has been established, burr holes over the hematoma are indicated to evacuate the clot.

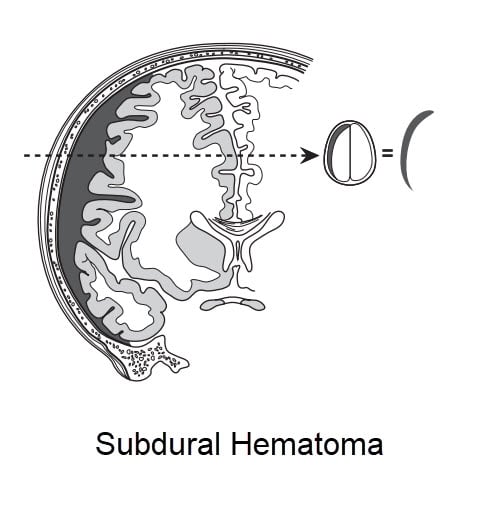
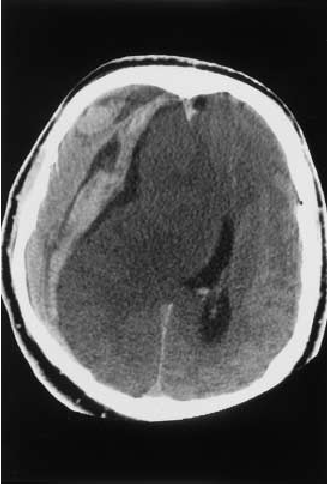
CT shows crescent-shaped, concave hyperdensity. Single arrows marked the spread of the subdural hematoma, and double arrows marked the midline shift.
Treatment of subdural hematomas depends on their severity. Treatment can range from watchful waiting to surgery.
- In small subdural hematomas with mild symptoms - no specific treatment other than observation. Repeated head imaging tests are often performed to monitor whether the subdural hematoma is improving.
- More severe subdural hematomas require surgery to reduce the pressure on the brain. Surgeons can use various techniques to treat subdural hematomas:
- Burr hole trephination. A hole is drilled in the skull over the area of the subdural hematoma, and the blood is suctioned out through the hole.
- Craniotomy. A larger section of the skull is removed to allow better access to the subdural hematoma and reduce pressure. The removed skull is replaced shortly after the procedure.
- Craniectomy. A section of the skull is removed for an extended period of time to allow the injured brain to expand and swell without permanent damage (rarely used).
 Osmosis Osmosis |
|
 |
Subdural Hematoma: This is an acute or chronic condition due to venous bleeding that builds up between the dura mater and the arachnoid layer. It often occurs in acceleration-deceleration whiplash injuries and may present days to weeks after the initial injury.
Play Video + QuizQuestion 1 |
12-year-old male gymnast with hemophilia A | |
20-year-old male suffering a head injury 2 hours ago | |
36-year-old female with head injury 30 minutes ago | |
55-year-old female with a cerebral aneurysm | |
78-year-old male with long-standing alcoholism |
Question 2 |
{kind=link}
Subarachnoid hemorrhage Hint: Subarachnoid hemorrhage typically occurs due to ruptured berry aneurysms and presents with the "worst headache" of a person's life. It does not present as crescent shaped on CT scan. | |
Subdural hematoma | |
Epidural hematoma Hint: Epidural hematomas may occur due to a laceration of the middle meningeal artery, and typically present with with a patient that had a lucid interval and suddenly looses consciousness. It also presents as biconvex on CT exam | |
Subgaleal hematoma Hint: Subgaleal hematomas typically present in neonates due to birth trauma, and present with subaponeurotic bleeding that crosses suture lines. | |
Caput succedaneum Hint: Caput succedaneum also typically present in neonates due to birth trauma with subcutaneous hemorrhage that crosses the suture lines. |
|
List |