The General Surgery End of Rotation Blueprint gastrointestinal and nutritional section includes 32 topics and represents 50% of your General Surgery EOR exam
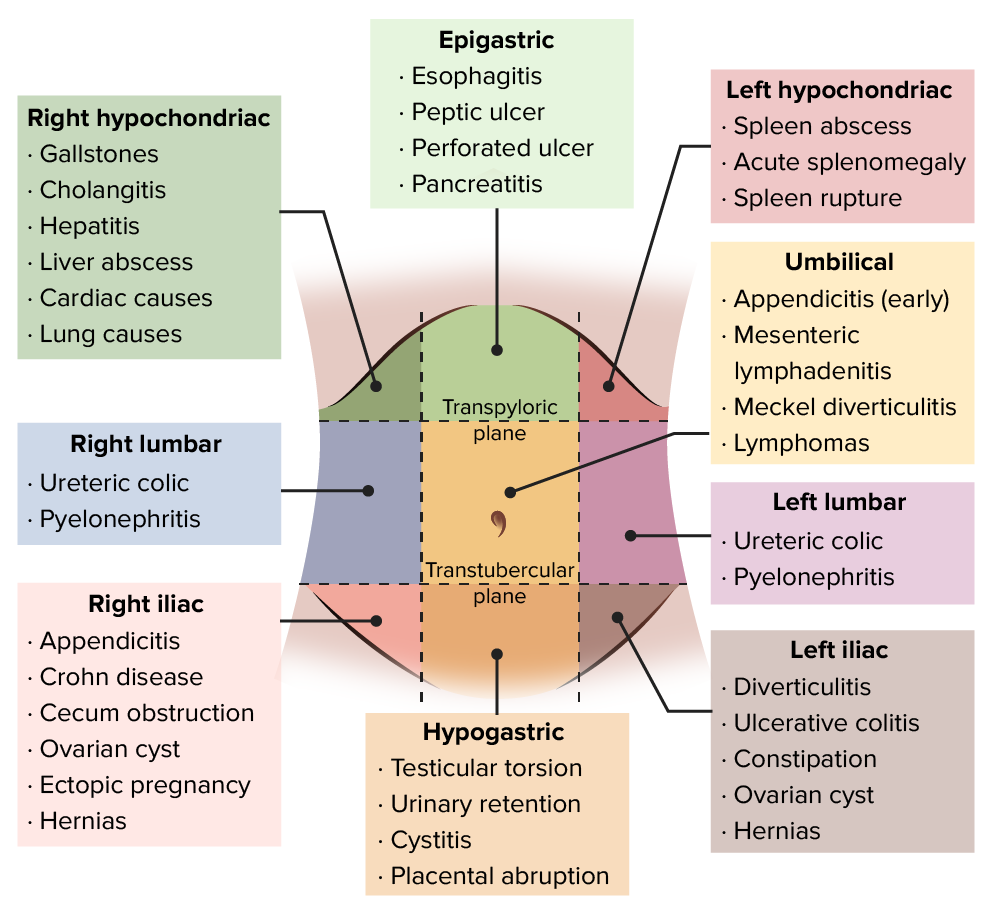
| Abdominal pain |
Flashcards ready when you areYou have opened several Quizlet sets recently. Loading this one only when needed helps prevent a temporary Quizlet limit.
EPIGASTRIC PAIN: PUD, gastritis, MI, pancreatitis, biliary colic, gastric volvulus, Mallory-Weiss RUQ PAIN: Cholecystitis, hepatitis, PUD, perforated ulcer, pancreatitis, liver tumors, gastritis, hepatic abscess, choledocholithiasis, cholangitis, pyelonephritis, nephrolithiasis, appendicitis (especially during pregnancy); thoracic causes (e.g., pleurisy/pneumonia), PE, pericarditis, MI (especially inferior MI). LUQ PAIN: PUD, perforated ulcer, gastritis, splenic injury, abscess, reflux, dissecting aortic aneurysm, thoracic causes, pyelonephritis, nephrolithiasis, hiatal hernia (strangulated paraesophageal hernia), Boerhaave’s syndrome, Mallory-Weiss tear, splenic artery aneurysm, colon disease. LLQ PAIN: Diverticulitis, sigmoid volvulus, perforated colon, colon cancer, urinary tract infection, small bowel obstruction, inflammatory bowel disease, nephrolithiasis, pyelonephritis, fluid accumulation from aneurysm or perforation, referred hip pain, gynecologic causes, appendicitis (rare). RLQ PAIN: Appendicitis! And same as LLQ; also mesenteric lymphadenitis, cecal diverticulitis, Meckel’s diverticulum, intussusception
|
| Acute and chronic cholecystitis | A 45-year-old woman with RUQ pain for 12 hours, fever, and leukocytosis
Presentation:
Diagnosis:
Treatment: Cholecystectomy |
| Acute and chronic pancreatitis | Epigastric pain radiating to back, with nausea and vomiting
Acute Pancreatitis - epigastric abdominal pain with radiation to the back and elevated lipase
 This 40-year-old woman complained of worsening epigastric pain of five days duration. On examination, she had hypotension, a board-like abdomen, and extensive ecchymosis over her right loin (Grey Turner’s sign)  Acute pancreatitis with Cullen’s sign Ranson’s criteria for poor prognosis: At admit:
At 48 hrs:
Treatment: IV fluids (best), analgesics, bowel rest Complication: pancreatic pseudocyst (a circumscribed collection of fluid rich in pancreatic enzymes, blood, and necrotic tissue) Chronic Pancreatitis - the classic triad of pancreatic calcification (plain abdominal x-ray), steatorrhea (high fecal fat), and diabetes mellitus
|
| Anal disease (fissures, abscess, fistula) | Excruciating pain with bowel movement (anal fissure)
Anorectal abscess is a result of infection, whereas fistula is a chronic complication of an abscess.
Treatment of abscess requires surgical drainage, followed by warm-water cleansing, analgesics, stool softeners, and a high-fiber diet are prescribed for all patients
Anorectal fistula is an open tract between two epithelium-lined areas and is associated with deeper anorectal abscesses
Fistula must be treated surgically Tearing rectal pain and bleeding which occurs with or shortly after defecation, bright red blood on toilet paper
Treatment:
|
| Anorexia | Think Appendicitis - Classic chronological order: 1. Periumbilical pain (intermittent and crampy) 2. Nausea/vomiting 3. Anorexia 4. Pain migrates to RLQ (constant and intense pain), usually in 24 hours
|
| Appendicitis | The first symptom is crampy or "colicky" pain around the navel (periumbilical)
Signs:
Clinical diagnosis:
TX: surgical appendectomy |
| Bariatric surgery | Guidelines for bariatric surgery which include:
BMI: body weight in kg divided by height in meters squared |
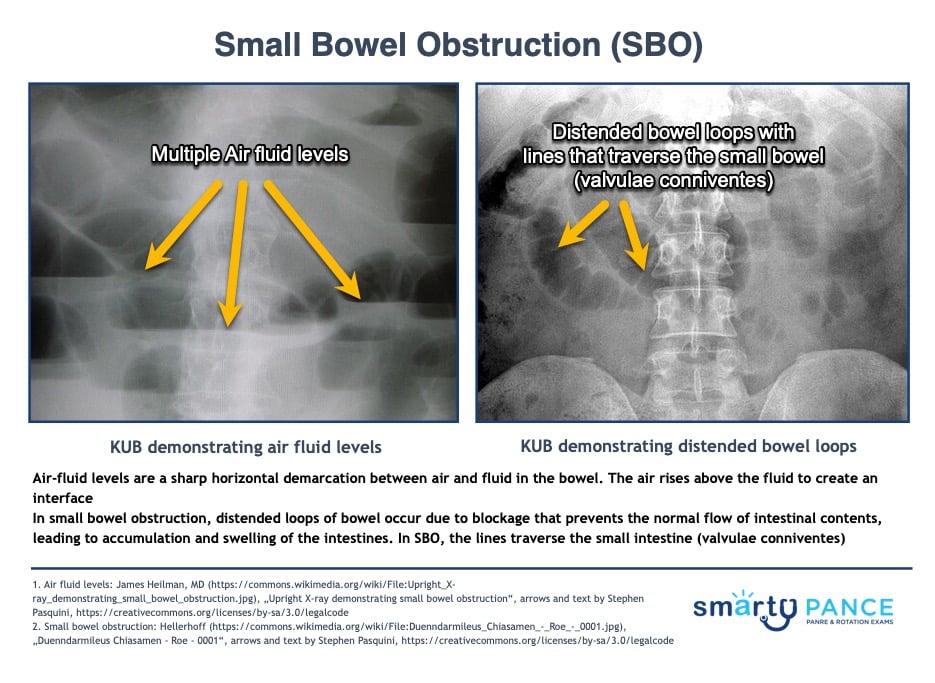
| Bowel obstruction (small, large, volvulus) | ReelDx Virtual Rounds (Small bowel obstruction)Patient with small bowel obstruction will present as → a 55-year-old male presents to the emergency department with a two-day history of severe abdominal pain, vomiting, and inability to pass stool or gas. He describes the pain as crampy and worsening, localized initially around the umbilicus but now diffused across the abdomen. His medical history is significant for an open appendectomy 20 years ago. On examination, his abdomen is distended and tender with high-pitched, tinkling bowel sounds. He is afebrile, but his heart rate is elevated. An abdominal X-ray reveals dilated loops of small bowel with air-fluid levels. You note valvulae conniventes across the full width of the bowel suggestive of a small bowel obstruction. A CT scan of the abdomen confirms the diagnosis, showing a transition point with no evidence of strangulation. The patient is admitted for nasogastric decompression, intravenous fluids, and bowel rest. Surgery is consulted for potential operative intervention, given his history of previous abdominal surgery and the likelihood of adhesive disease. The patient is closely monitored for signs of bowel ischemia or perforation.
DX: Obtain plain radiographs to quickly confirm a diagnosis of bowel obstruction, and, provided the films do not have findings that indicate the need for immediate intervention, then use computed tomography (CT) of the abdomen and pelvis to further characterize the nature, severity, and potential etiologies of the obstruction
TX: Treat with decompression with an NGT, surgery if a mechanical obstruction is suspected
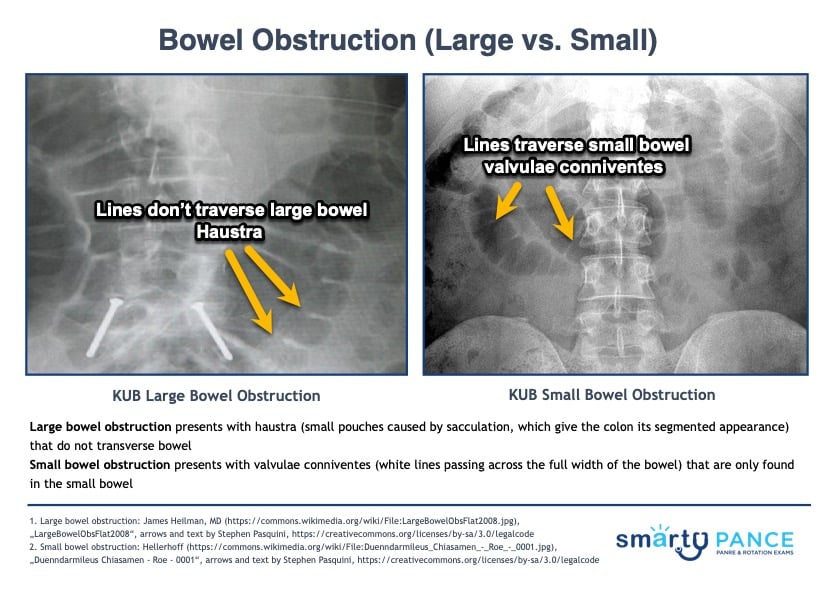
Hyperactive bowel sounds, as heard in SBO Patient with large bowel obstruction will present as → a 70-year-old female presents to the emergency department with a three-day history of worsening abdominal distension, constipation, and intermittent, crampy abdominal pain. She reports her last bowel movement was four days ago, which was smaller in caliber than usual. She has a history of chronic constipation and a 20-pound unintentional weight loss over the past six months. On examination, her abdomen is markedly distended, tympanic to percussion, and tender on palpation, particularly in the lower quadrants. No bowel sounds are heard on auscultation. Her vital signs show mild tachycardia but are otherwise stable. An abdominal X-ray reveals dilated loops of large bowel with haustra and a “cut-off” sign in the sigmoid region. A CT scan of the abdomen and pelvis confirms a large bowel obstruction with a suspected mass in the sigmoid colon. The patient is admitted for nasogastric decompression, intravenous fluids, and bowel rest. Surgery and gastroenterology are consulted for further evaluation, including potential colonoscopy and biopsy of the mass. The patient is counseled about the likelihood of colorectal cancer as a potential underlying cause and the need for surgical intervention.
DX: Obtain plain radiographs to quickly confirm a diagnosis of bowel obstruction, and, provided the films do not have findings that indicate the need for immediate intervention, then use computed tomography (CT) of the abdomen and pelvis to further characterize the nature, severity, and potential etiologies of the obstruction
TX: Bowel rest, NG tube placement, surgery as directed by the underlying cause  KUB in LBO demonstrates dilated loops of the large bowel with haustra (lines that don't traverse the large bowel) and air-fluid levels in the large intestine SBO vs. LBO On the physical exam:
On the abdominal x-ray (KUB):
|
| Cholangitis | RUQ pain, jaundice, and fever
Cholangitis is a complication of gallstones with symptoms secondary to an infected obstruction of the common bile duct (E.coli is the #1 cause)
ERCP is the optimal procedure both for diagnosis and for treatment |
| Cholelithiasis and choledocholithiasis | A precursor to cholecystitis, cholesterol stones account for > 85% of gallstones in the Western world |
| Colorectal carcinoma | Painless rectal bleeding and a change in bowel habits in a patient 50-80 years of age
Tx: resection and adjuvant chemotherapy Colon cancer screening for average-risk patients should begin at 45 years and end at 75 years of age
USPSTF colorectal cancer screening guidelines **When adequate screening colonoscopy is accomplished, intercurrent stool tests (i.e., between colonoscopy examinations) are not necessary. In addition, for patients who have had a negative colonoscopy and have been recommended to have routine screening in 10 years, screening with FIT or other screening tests is not indicated prior to the end of the 10-year period. **There is adequate evidence that the benefits of detection and early intervention decline after age 75 years |
| Diarrhea, constipation, obstipation, and change in bowel habits | Constipation: Defined as less than 2 bowel movements per week
Obstipation is a severe form of constipation, where a person cannot pass stool or gas
Illeus
Gastroparesis
Pseudomembranous colitis
|
| Diverticular disease | LLQ pain, tenderness, abdominal distention, fever and leukocytosis in older patients
Inflammation of an abnormal pouch (diverticulum) in the intestinal wall, usually found in the large intestine. The presence of the pouches themselves is called diverticulosis. When they become inflamed, the condition is known as diverticulitis.
DX: Diagnose using abdominal and pelvic CT with oral, rectal, and IV contrast; do colonoscopy 1 to 3 months after the episode to look for cancer.
TX: Management depends on severity but typically includes conservative management (pain control + liquid diet x 2-3 days), sometimes antibiotics, and sometimes percutaneous or endoscopic ultrasound-guided drainage or surgical resection
|
| Esophageal cancer | Progressive dysphagia to solid foods along with weight loss, reflux, and hematemesis
Adenocarcinoma:
Squamous cell:
|
| Esophageal Strictures | Solid food dysphagia in a patient with a history of GERD
Symptoms
Esophageal achalasia: primary esophageal motility disorder characterized by the absence of lower esophageal peristalsis.
DX: Barium swallow shows there is acute tapering at the lower esophageal sphincter and narrowing at the gastroesophageal junction, producing a "Bird’s beak" or "rat's tail" appearance - distal 2/3 most common
TX: EGD dilation of the esophagus or myotomy is the preferred treatment Esophageal web: thin membranes in the mid-upper esophagus. May be congenital or acquired Plummer-Vinson: esophageal webs + dysphagia + iron deficiency anemia A Schatzki ring is a diaphragm-like mucosal ring that forms at the esophagogastric junction (the B ring). If the lumen of this ring becomes too small, symptoms occur |
| Gastric cancer | Present with weight loss, abdominal fullness/pain, anemia, early satiety, melena, anorexia, guaiac-positive stool
|
| Heartburn and dyspepsia | Dyspepsia and abdominal pain are common indicators of gastritis
Three causes: 1. Autoimmune or hypersensitivity reaction (e.g. pernicious anemia)
2. Infection - H. pylori (most common)
3. Inflammation of the stomach lining (NSAIDS and Alcohol)
Peptic ulcer disease Etiology: H. pylori (most common), NSAID use, Zollinger-Ellison syndrome (refractory PUD) - gastrin-secreting tumor
Diagnosis: Endoscopy with biopsy is the gold standard for diagnosis Treatment:
|
| Hematemesis |
|
| Hemorrhoids |
Flashcards ready when you areYou have opened several Quizlet sets recently. Loading this one only when needed helps prevent a temporary Quizlet limit.
Hemorrhoids are varicose veins of the anus and rectum
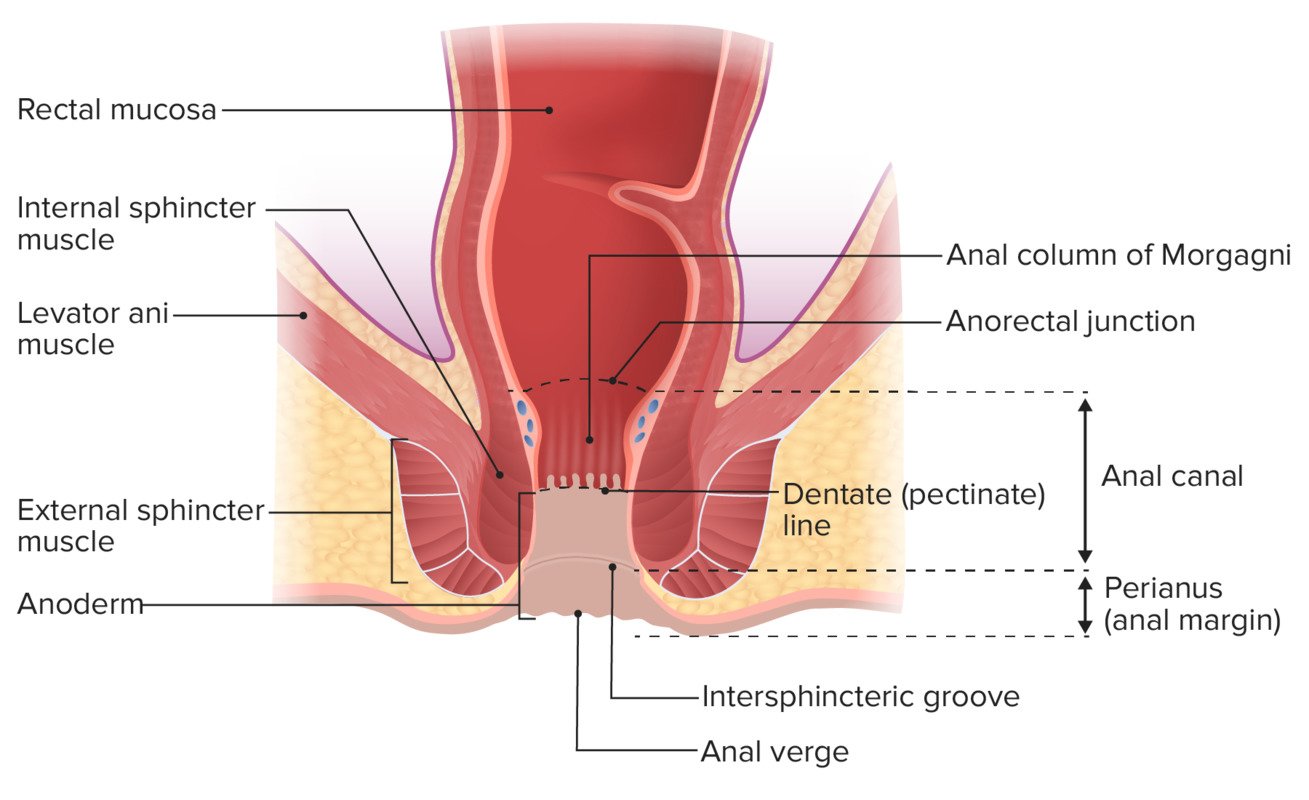
External hemorrhoids - lower 1/3 of the anus (below dentate line) Patient with external hemorrhoids will present as → a 35-year-old female presents with anal pain and itching, especially during sitting and following bowel movements. She recently gave birth to her second child. On examination, there are swollen, bluish, tender lumps around the anal verge, consistent with thrombosed external hemorrhoids. She is advised on warm sitz baths and is prescribed a topical anesthetic cream for symptomatic relief. She is also educated on the importance of avoiding straining and maintaining soft bowel movements through adequate hydration and fiber intake. She is informed that the thrombosed hemorrhoids may resolve spontaneously, but surgical intervention can be considered if symptoms persist or worsen.
 Thrombosed external hemorrhoid Internal hemorrhoids - upper 1/3 of the anus (above the dentate line) Patient with internal hemorrhoids will present as → a 42-year-old male presents with painless rectal bleeding during bowel movements for the past week. He reports a history of chronic constipation. On examination, there is no visible perianal abnormality. Digital rectal examination is unremarkable, but there is evidence of bright red blood on the glove. An anoscopy reveals enlarged, non-prolapsing internal hemorrhoids. The patient is counseled on dietary modifications, including increased fiber intake and hydration, to alleviate constipation. He is also prescribed a topical hemorrhoidal cream with hydrocortisone and instructed on the importance of regular bowel habits to prevent straining.
Classification of internal hemorrhoids is based on the degree of prolapse
 Grade IV internal Hemorrhoids |
| Hepatic carcinoma | Abdominal pain, weight loss, right upper quadrant mass
Etiology: Cirrhosis, Hepatitis B, Hepatitis C, Hepatitis D, Aflatoxin from Aspergillus
Treatment: Resection, Transplant - Poor prognosis |
| Hernias (inguinal, femoral, incisional) | Inguinal hernias:
Ventral: Often from previous abdominal surgery, obesity. Abdominal mass noted at the site of previous incision. Umbilical hernia: Very common, generally is congenital and appears at birth. Many umbilical hernias resolve on their own and rarely require intervention. Refer to surgery if an umbilical hernia persists >2 years of life. Strangulated: Hernia becomes strangulated when the blood supply of its contents is seriously impaired. Obstructed: This is an irreducible hernia containing intestine that is obstructed from without or within, but there is no interference to the blood supply to the bowel. Incarcerated: Hernia so occluded that it cannot be returned by manipulation, it may or may not become strangulated. |
| Hiatal hernia | 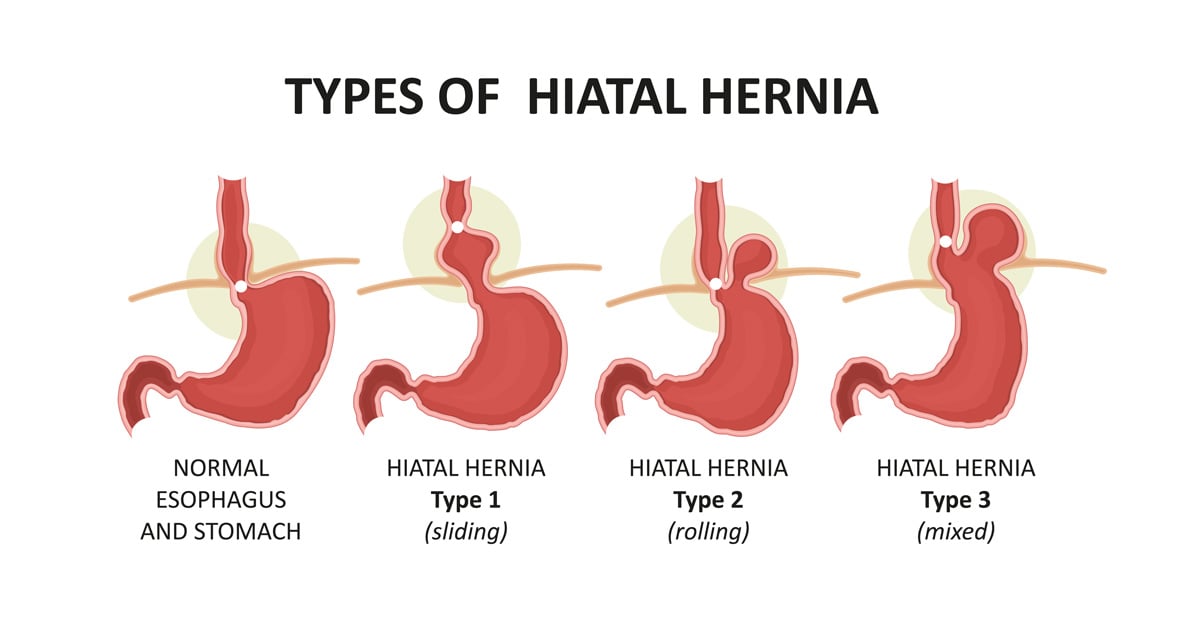
Hiatal (diaphragmatic): Involves protrusion of the stomach through the diaphragm via the esophageal hiatus.
Tx: acid reduction may suffice, although surgical repair can be used for more serious cases. |
| Inflammatory bowel disease | 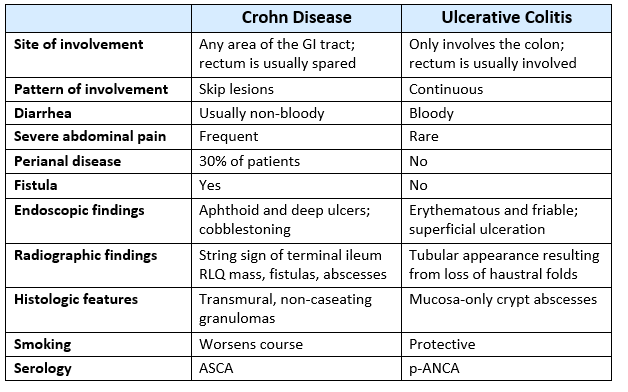
Ulcerative Colitis Ulcerative colitis will present as → a 32-year-old woman comes to your office with a 6-month history of loose bowel movements, approximately eight per day. Blood has been present in many of them. She has lost 30 pounds. For the past 6 weeks, she has had intermittent fever. She has had no previous gastrointestinal (GI) problems, and there is no family history of GI problems. On examination, the patient looks ill. Her blood pressure is 130/ 70 mm Hg. Her pulse is 108 beats/ minute and regular. There is generalized abdominal tenderness with no rebound. A sigmoidoscopy reveals a friable rectal mucosa with multiple bleeding points. Isolated to the colon starts at the rectum and moves proximally
Treatment:
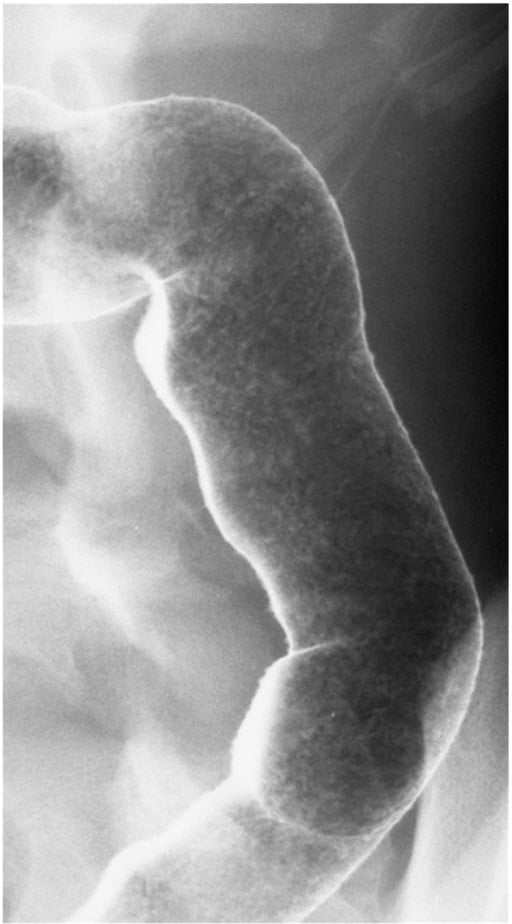 Lead pipe appearance on Double-contrast barium enema. Image by Division of Gastroenterology and Hepatology, Mayo Clinic College of Medicine, Rochester, MN, USA. License: CC BY 3.0 Crohn's disease Crohn’s disease will present as → a 25-year-old man with an 18-month history of chronic abdominal pain. The patient has seen several physicians and has been diagnosed as having a “nervous stomach,” irritable bowel syndrome, and “depression.” Associated with this abdominal pain for the past 3 months have been nonbloody diarrhea, anorexia, and a weight loss of 20 pounds. He has developed a painful area around the anus. On examination, the patient has diffuse abdominal tenderness. He looks thin and unwell. He has a tender, erythematous area in the right perirectal area. From mouth to anus, transmural, skip lesions, and cobblestoning!
Treatment:
 Stenosis of the colon with cobblestoning particular to Crohn's disease |
| Jaundice | Serum bilirubin > 2.5 mg/dl
Causes of postoperative jaundice: Prehepatic: Hemolysis (prosthetic valve), resolving hematoma, transfusion reaction, post cardiopulmonary bypass, blood transfusions (decreased RBC compliance leading to cell rupture) Hepatic: Drugs, hypotension, hypoxia, sepsis, hepatitis, “sympathetic” hepatic inflammation from adjacent right lower lobe infarction of the lung or pneumonia, preexisting cirrhosis, right-sided heart failure, hepatic abscess, pylephlebitis (thrombosis of portal vein), Gilbert syndrome, Crigler-Najjar syndrome, Dubin-Johnson syndrome, fatty infiltrate from TPN Posthepatic: Choledocholithiasis, stricture, cholangitis, cholecystitis, biliary-duct injury, pancreatitis, sclerosing cholangitis, tumors (e.g., cholangiocarcinoma, pancreatic cancer, gallbladder cancer, metastases), biliary stasis (e.g., ceftriaxone [Rocephin®]) |
| Melena and hematochezia | Melena: black, tarry stool - upper GI bleed
Hematochezia: bright red blood per rectum (BRBPR) - lower GI bleed
|
| Nausea and vomiting | Postoperative nausea and vomiting (PONV) is an unpleasant complication affecting 30 percent of children and adults after anesthesia
Nausea can have causes that aren't due to underlying disease. Examples include motion such as from a car and plane, taking pills on an empty stomach, eating too much or too little, or drinking too much alcohol
|
| Pancreatic carcinoma | An elderly man with large nontender palpable gallbladder (Courvoisier's sign)
Painless jaundice is pathognomonic
Presentation:
DX:
TX:
 The Whipple procedure involves removing the antrum of the stomach, part of the duodenum, the head of the pancreas, and gallbladder  CT with IV contrast showing pancreatic adenocarcinoma at the head of the pancreas. |
| Pancreatic pseudocyst | Pancreatitis and a palpable epigastric mass
Treatment - if pseudocyst persists for 4 to 6 weeks or continues to enlarge
|
| Peptic ulcer disease | PUD is an ulcer of the upper GI tract mucosa involving the proximal duodenum (90%) and distal stomach (10%). There are 2 main types of ulcers duodenal and gastric
Duodenal ulcer (food classically decreases pain think Duodenum = Decreased pain with food)
Gastric ulcer (food classically causes pain)
Bleeding — Acute upper gastrointestinal hemorrhage is the most common complication of peptic ulcer disease DX: Upper endoscopy is the most accurate diagnostic test for peptic ulcer disease
TX: All patients with peptic ulcers should receive antisecretory therapy with a proton pump inhibitor (PPI) (eg, omeprazole 20 to 40 mg daily or equivalent) for 4-8 weeks
|
| Pyloric stenosis | An infant with projectile vomiting
ReelDx Virtual Rounds (Pyloric stenosis)Pyloric stenosis is a congenital condition where a newborn’s pylorus undergoes hyperplasia and hypertrophy, leading to obstruction of the pyloric valve which causes vomiting (that might be projectile), as well as dehydration and metabolic alkalosis Projectile vomiting occurs shortly after feeding in an infant < 3 mo. old with a palpable “olive-like” mass at the lateral edge of the right upper quadrant
DX: Diagnosis is by ultrasound
TX: surgical correction - pyloromyotomy (Ramstedt's procedure)  Pyloric stenosis as seen on ultrasound in a 6-week-old. Notice the "double track" (red arrow) |
| Small bowel carcinoma | The most common presenting symptom of a small bowel tumor is abdominal pain- typically intermittent and crampy in nature
Treatment is surgery — Localized adenocarcinomas of the small bowel are best managed with wide segmental surgical resection
|
| Toxic megacolon | Patient will present as → a 24-year-old man with ulcerative colitis who receives Lomotil for excessive diarrhea and develops a fever, abdominal pain, and tenderness, and a massively dilated colon on abdominal x-ray. A complication of ulcerative colitis (most common), Crohn’s, Hirschsprung’s, pseudomembranous colitis, enteritis
DX: Toxic megacolon is diagnosed based on clinical signs of systemic toxicity combined with radiographic evidence of colonic dilatation (diameter >6 cm) The most widely used criteria for the clinical diagnosis of toxic megacolon are:
TX: Decompression of the colon is required
 Toxic Megacolon seen in ulcerative colitis. The patient underwent a colectomy. |



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}