Patient will present as → a 67-year-old male with a history of hypertension, hyperlipidemia, and a 30-pack-year smoking history presents to the clinic complaining of pain in his calves when he walks more than two blocks, which is relieved by rest. He notes that this pain has been progressively worsening over the past six months, limiting his ability to walk long distances. He denies any rest pain or non-healing wounds on his feet. On examination, his pulses are diminished in both feet, and his ankle-brachial index (ABI) is 0.6 on the right and 0.65 on the left, indicating moderate peripheral arterial disease. His toes are cool to touch, but there are no signs of ulceration or gangrene. Doppler ultrasound confirms significant stenosis in the bilateral superficial femoral arteries. The patient is diagnosed with claudication secondary to peripheral arterial disease. He is counseled on smoking cessation and started on a supervised exercise program to improve his walking distance. He is also prescribed a statin and an antiplatelet agent for atherosclerotic disease management. A referral to a vascular surgeon is made for consideration of revascularization options, given his lifestyle-limiting symptoms.
Claudication derives from the Latin word claudicare which means “to limp.” It is caused by a reduction in blood flow to the leg muscles, most commonly by an atherosclerotic plaque.
- It is not due to a blood clot or embolization. The reduced arterial blood supply cannot meet the metabolic demand of the muscles utilized during walking.
The diagnosis can readily be suspected based on the three-part definition obtained by history:
- pain in the leg with walking
- relieved within a few minutes of rest
- reproducible at the same walking distance each time
Claudication is a symptom of peripheral arterial disease (PAD)
- PAD most often affects the lower extremities and, less commonly, the upper extremities and the intestinal and renal arteries.
- It is usually caused by atherosclerosis.
- It leads to a gradual slowly developing reduction in blood flow in the extremities (chronic limb ischemia).
The main risk factors for PAD include smoking, diabetes, hypertension, hypercholesterolemia, advanced age, male gender, obesity, sedentary lifestyle, family history of vascular disease, heart attack, and stroke.
PAD causes a progressive loss of blood supply to the leg. The calf muscles atrophy; hair appendages die (hair loss), as do sweat glands (dry scaly skin); the skin thins out (shiny), and ulcers may develop. Capillary refill time becomes prolonged (normal is ≤ 2 s).
Watch Out
Always ask about rest pain, as the presence of rest pain identifies a patient as having limb-threatening ischemia.
PAD is Defined as an ABI < 0.9. The ABI Confirms the Diagnosis of PAD, Gives an Indication of Severity, and is a Useful Tool to Follow Progression
- Normal ABI 1.2–1.0
- Mild disease 0.9–0.7
- Moderate disease 0.7–0.4
- Severe disease/rest pain <0.4
Angiography is considered the gold standard for diagnosing PAD/PVD
- A-gram (arteriogram: dye in vessel and x-rays) maps disease and allows for best treatment option (i.e., angioplasty vs. surgical bypass vs. endarterectomy)
Platelet inhibitors: Cilostazol, Aspirin, Clopidogrel
- Treat lipids - Statins
- Revascularization with PTA, bypass grafts, stenting
- Exercise - walking to the point of claudication
***βblockers are contraindicated in isolated PAD – it will worsen claudication!
Treatment options for severe PVD:
- Surgical graft bypass
- FEM-POP bypass: Bypass SFA occlusion with a graft from the FEMoral artery to the POPliteal artery
- FEM-DISTAL bypass: Bypass from the FEMoral artery to a DISTAL artery (peroneal artery, anterior tibial artery, or posterior tibial artery)
- Angioplasty—balloon dilation
- Endarterectomy—remove diseased intima and media
- Surgical patch angioplasty (place patch over stenosis)
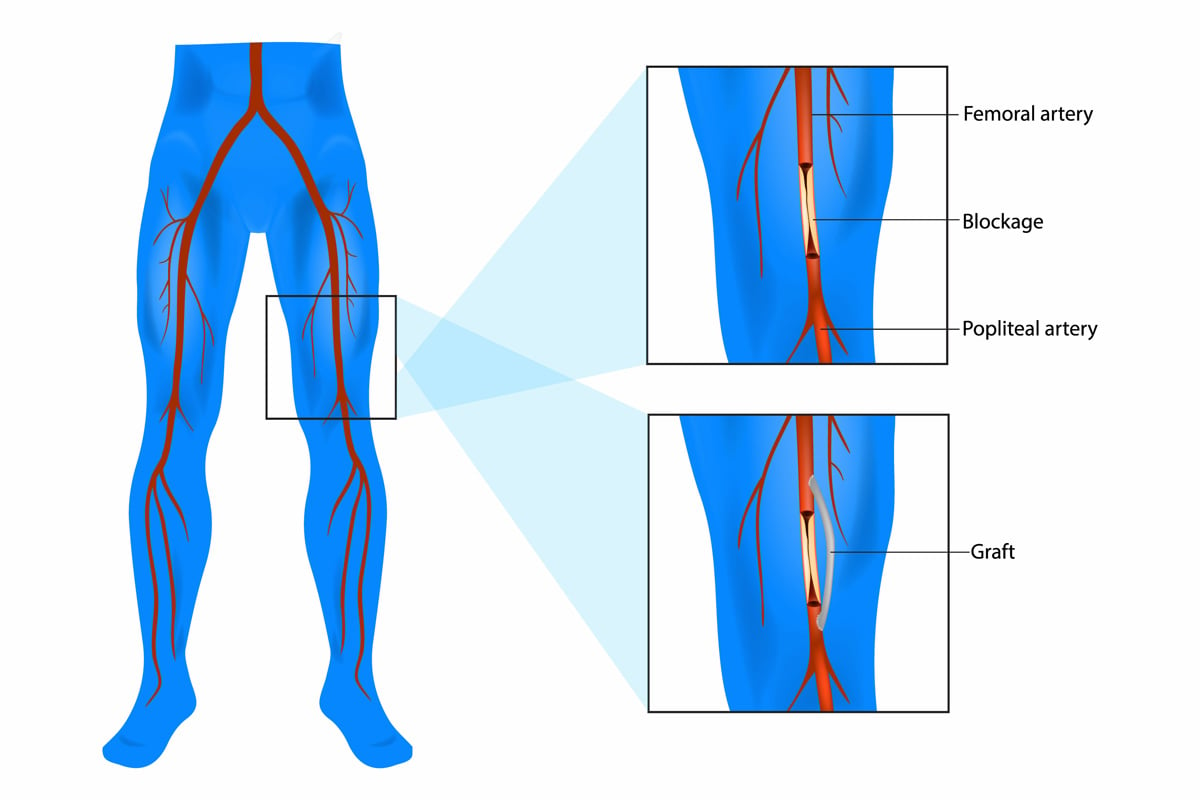
Femoral popliteal (also called femoropopliteal or Fem-Pop) bypass surgery
What graft material has the longest patency rate?
- Autologous vein graft
What is an “in situ” vein graft?
- The saphenous vein is more or less left in place, all branches are ligated, and the vein valves are broken with a small hook or cut out; a vein can also be used if reversed so that the valves do not cause a problem
Question 1 |
Deep vein thrombosis (DVT) Hint: DVT typically presents with unilateral leg swelling, pain, and erythema. The pain associated with DVT does not typically resolve with rest and is not induced by walking. | |
Peripheral arterial disease (PAD) | |
Chronic venous insufficiency Hint: This condition usually presents with leg swelling, varicose veins, skin changes, and possibly ulceration. It does not typically cause pain that resolves with rest or is induced by walking. | |
Lumbar spinal stenosis Hint: While lumbar spinal stenosis can cause leg pain with walking (neurogenic claudication), it is often associated with back pain and the pain may be relieved by leaning forward or sitting. The absence of back pain and the presence of diminished pulses are more indicative of PAD. | |
Achilles tendinitis Hint: Achilles tendinitis presents with pain localized to the back of the ankle and is associated with physical activity. It does not cause pain that resolves with rest or is induced by walking and is not associated with diminished pulses. |
References: UpToDate