

12-month-old with episodic abdominal pain and vomiting (View Case)
Patient will present as → a 10-month-old previously healthy male is brought to the emergency department by his parents with a 12-hour history of intermittent episodes of severe, inconsolable crying, during which he draws his knees to his chest. Between episodes, he appears fatigued but consolable. His parents report two episodes of non-bilious vomiting, and more recently, they noticed a bloody, mucousy stool described as “currant jelly”. He has no recent travel, fever, or sick contacts. On exam, he appears pale and lethargic. His abdomen is soft but mildly distended with a palpable sausage-shaped mass in the right upper quadrant. An abdominal ultrasound reveals a target sign, confirming the diagnosis of intussusception. Management includes fluid resuscitation and air enema reduction, with surgical intervention if nonoperative reduction fails.Intussusception is the invagination of a proximal segment of the bowel into the portion just distal to it.
- It occurs most commonly in children (95% of cases), generally following a viral infection
- Ileocolic intussusception involves the ileocecal junction and accounts for 90 percent of all cases
- In adults, intussusception is almost always caused by a neoplasm
- The initial symptoms are the sudden onset of significant, colicky abdominal pain that recurs every 15 to 20 minutes, often with vomiting
- Paroxysmal abdominal pain is the main symptom. The child appears relatively well between episodes or may appear lethargic
- A sausage-like mass may be felt on abdominal exam
- Later, as intestinal ischemia develops, pain becomes steady, the child becomes more lethargic, and mucosal hemorrhage causes heme-positive stool on rectal examination and sometimes the spontaneous passage of a currant jelly stool
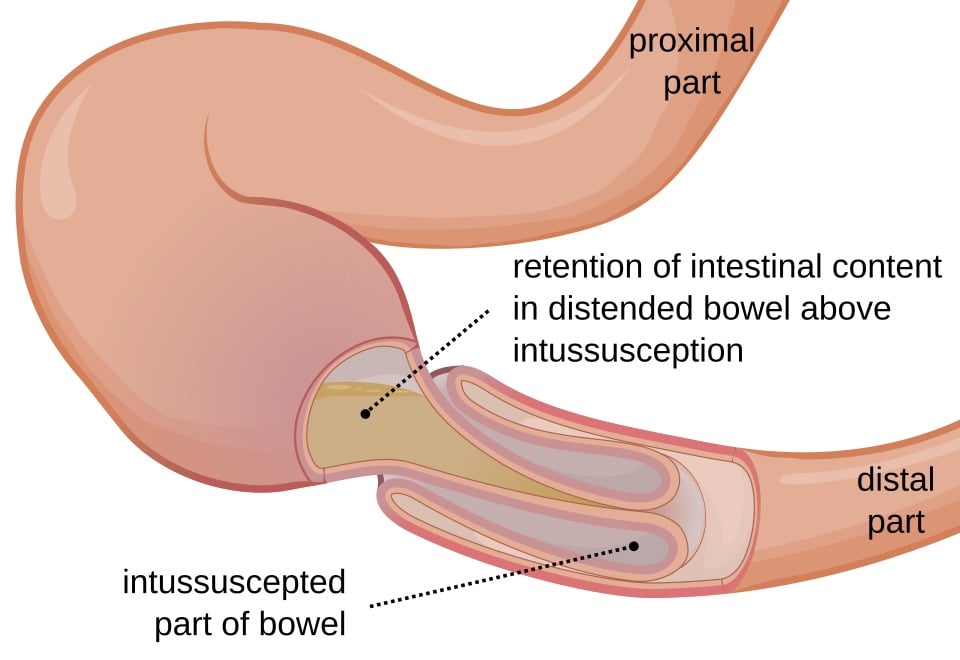
Intussusception with telescoping of one segment of bowel into another. Illustration by Olek Remesz via Wikimedia Commons, CC BY-SA 3.0.
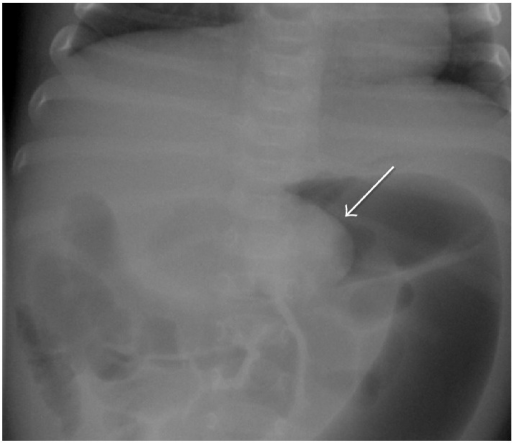
Diagnosis is made with abdominal ultrasound, showing the classic “target” or “donut” sign
- For children, an air or contrast enema may be both diagnostic and therapeutic
- For adults, barium enema should not be used, and abdominal plain-film radiography shows nonspecific obstruction. CT is the best means of establishing the diagnosis in adults, but many cases are diagnosed only at surgery
- An abdominal x-ray will reveal a “crescent" or "meniscus sign” or a “Bull's eye/target sign/coiled spring lesion” representing layers of the intestine within the abdomen

Air or contrast enema reduction may be curative for children; if not, surgery is needed
- The intussusceptum can be successfully reduced in 75 to 95% of children
- If the air enema is successful, children are observed overnight to rule out occult perforation
- If the reduction is unsuccessful or if the intestine has perforated, immediate surgery is required
- Adults generally require surgery
- When reduction is achieved without surgery, the recurrence rate is 5 to 10%
 Osmosis Osmosis |
|
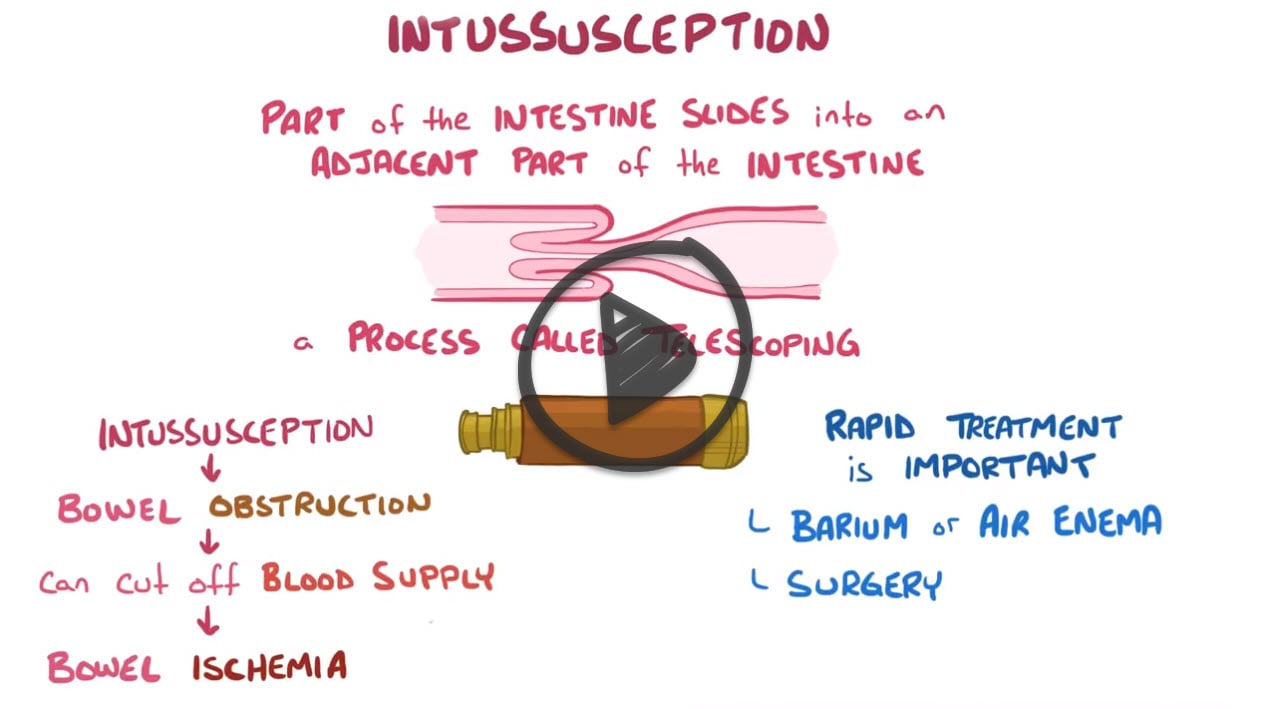 |

Intussusception is the most common cause of intestinal obstruction in children between the ages of 3 months and 3 years. It is more common in boys and presents with episodic abdominal pain along with diarrhea. Patients have characteristic red, currant jelly stools, while physical exam findings can include a sausage-shaped mass. Conservative treatment of this disorder involves air or barium enema, while surgical reduction may be done for complicated or refractory cases, as this is a potentially life-threatening issue.
Play Video + QuizQuestion 1 |
Acute appendicitis Hint: Doesn’t lead to passage of red-currant jelly stool and no mass at the right upper quadrant. | |
Intussusception | |
Acute gastric volvulus Hint: Presents as abdominal pain, retching and inability to pass a nasogastric tube. | |
Gastroenteritis Hint: Diarrhoea is more prominent. Although the stools may contain blood and mucus, they are fecal and bile-stained.
|
Question 2 |
Passage of nasogastric tube placed for decompression Hint: See D for explanation | |
Placing an intravenous line for rehydration. Hint: See D for explanation | |
Starting intravenous antibiotics. Hint: See D for explanation | |
Hydrostatic barium enema. |
Question 3 |
Barium enema Hint: Barium enema shows a filling defect at the apex of the intussusception and a typical coiled-spring appearance of barium between the intussuscipiens and intussusceptum. | |
Abdominal Ultrasonography | |
Abdominal radiograph Hint: In early cases, plain abdominal X-rays often show absence of gas shadow in the right colon but air-fluid levels in the small bowel in the erect film and gaseous distension of ileal loops in the supine film. | |
None of the above Hint: See B for explanation |
Question 4 |
Barium enema | |
Abdominal ultrasonography Hint: Is mostly used as the first-line diagnostic test for suspected intussusceptions, but is not the gold standard. | |
Abdominal radiograph Hint: Plain abdominal radiograph reveals signs that suggest intussusceptions in only 60% of cases. | |
None of the above |
Question 5 |
Pneumatic reduction under fluoroscopy using air as a contrast medium is a treatment option. Hint: See C for explanation | |
Hydrostatic reduction is contraindicated if the child has signs of peritonitis or gangrenous bowel. Hint: See C for explanation | |
In adults, intussusception almost always is caused by viral infection. | |
Intussusception is the invagination of a segment of bowel into another immediately adjacent to it. Hint: See C for explanation |
|
List |
References: Merck Manual · UpToDate