Patient will present as → a 61-year-old healthy man undergoes a screening colonoscopy. He exercises daily, does not use tobacco, bloody or dark stools, changes in stool, abdominal pain, or fatigue. His prior colonoscopy 10 years ago was normal. During today’s colonoscopy, his gastroenterologist notes a small pedunculated growth in the descending colon.
Colonic polyps are a small clump of cells that forms on the lining of the colon or rectum. Most are harmless. But some can develop into cancer.
- Colonic polyps are common; the incidence ranges from 7% to 50% (depending on the diagnostic method used)
- The main concern is malignant transformation, which occurs at different rates depending on the size and type of polyp

"In patients with polyps, aspirin and COX-2 inhibitors may help prevent formation of new polyps."
- Colonic polyps are the most common cause of painless rectal bleeding in the pediatric population
- Adenomatous polyps are common in the distal colon and rectum
- Polyps of the distal colon are commonly benign if seen in the proximal colon they are more likely to be cancerous
- The larger the colonic polyp, the greater the risk of malignant transformation
- Villous adenomas have a 30-70% risk of malignant transformation
- The greater the number of concomitant colonic polyps, the greater the risk of malignant transformation
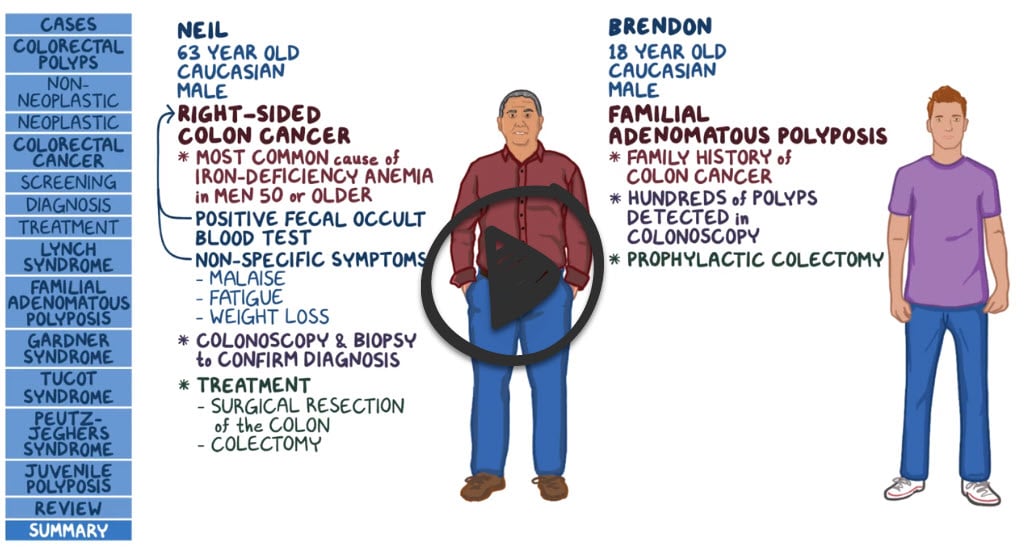
Familial adenomatous polyposis (FAP) - is characterized by the development of hundreds to thousands of colonic adenomatous polyps
- Colorectal polyps develop by a mean age of 15 years and cancer at 40 years.
- First-degree relatives of patients with FAP should undergo genetic screening after age 10 years.
- The family should undergo yearly sigmoidoscopy beginning at 12 years of age.
Colonoscopy is the recommended diagnostic and therapeutic procedure
- Diagnosis is by colonoscopy and biopsy
- Once identified, follow-up colonoscopy in 3-5 years

Colon polyp on a short stalk
Polyps should be removed completely with a snare or electrosurgical biopsy forceps during total colonoscopy
- Complete excision is particularly important for large villous adenomas, which have a high potential for cancer
- If colonoscopic removal is unsuccessful, laparotomy should be done
First surveillance:
- Individuals with an advanced adenoma should undergo a first surveillance colonoscopy in three years
- For adenomas ≥20 mm that have been resected piecemeal, repeat colonoscopy should be performed at six months
- If only one or two small (<10 mm) tubular adenomas are found on baseline colonoscopy, the first surveillance colonoscopy should be performed in 7 to 10 years
Subsequent surveillance:
- The timing of the subsequent surveillance colonoscopy is based on the findings of the first surveillance colonoscopy (see UpToDate)
 Osmosis Osmosis |
|
 |
Question 1 |
the presence of more than 100 colorectal adenomas. | |
the presence of more than 10 colorectal adenomas. Hint: See A for explanation | |
the presence of more than 1000 colorectal adenomas. Hint: See A for explanation | |
the presence of more than 1 colorectal adenomas. Hint: See A for explanation |
Question 2 |
follow-up colonoscopy in 1-2 years. | |
follow-up colonoscopy in 3-5 years. | |
follow-up colonoscopy in 5-7 years. | |
follow-up colonoscopy in 10 years |
Question 3 |
Aspirin Hint: See E for explanation | |
Cox-2 inhibitors Hint: See E for explanation | |
Propranolol Hint: See E for explanation | |
Metformin Hint: See E for explanation | |
both a and b |
Question 4 |
every 1-2 years beginning at age 19-21 Hint: See B for explanation | |
every 1-2 years beginning at age 10-12 years old | |
once at age 10 then every 10 years afterwards Hint: See B for explanation | |
at first signs of symptoms Hint: See B for explanation |
|
List |
References: Merck Manual · UpToDate